
![]()
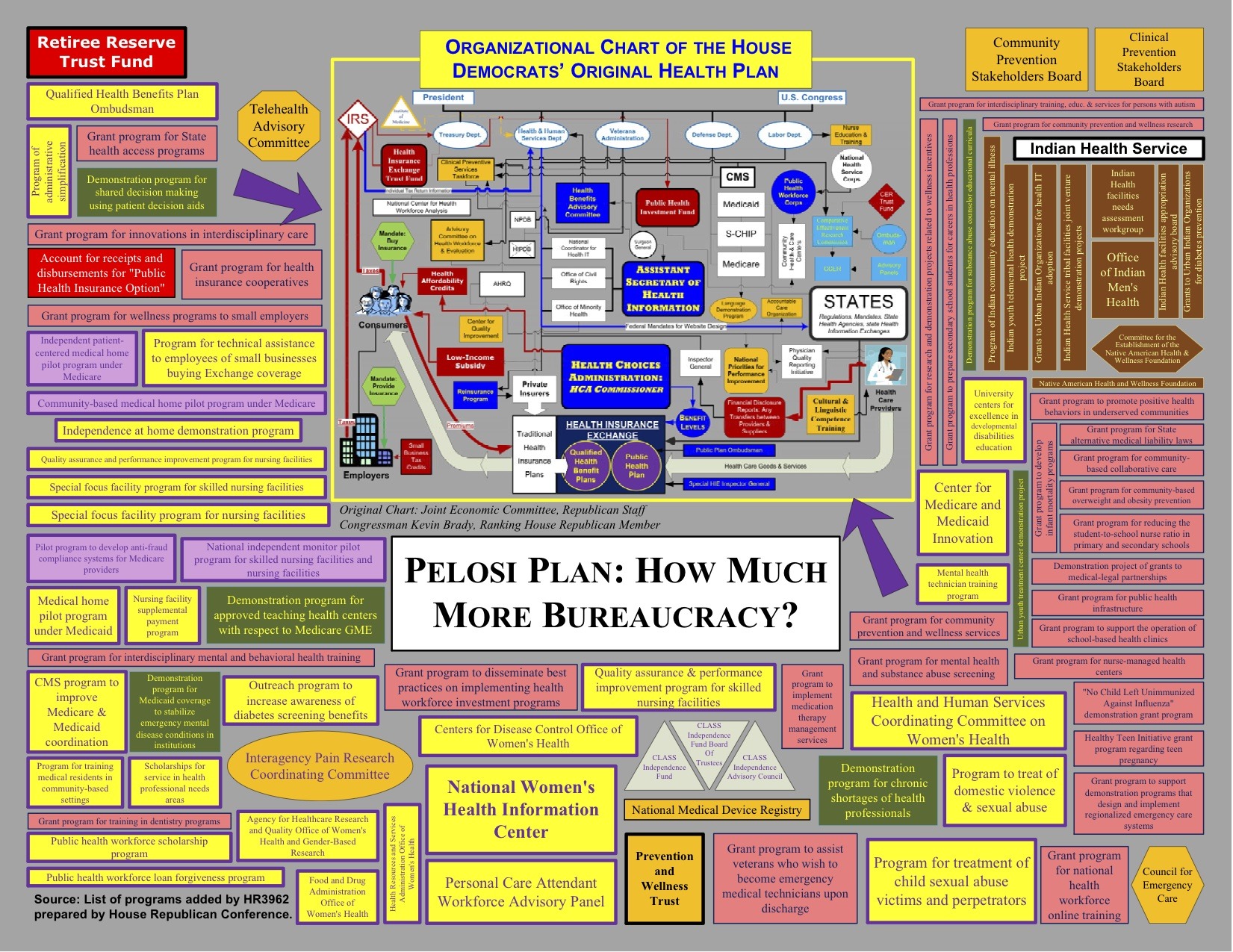
Tom Blumer from BizzyBlog has updated his map of the ObamaCare/PelosiCare behemoth and what it creates. Namely 111 agencies, regulators, committees, boards and offices: (click on picture to enlarge)
Meanwhile Senator Gregg reacts to the new CBO estimate:
Senator Judd Gregg (R-NH), ranking member of the Senate Budget Committee today commented on the Congressional Budget Office’s (CBO) more detailed cost estimate of the manager’s amendment to the House health reform bill.
Senator Gregg stated, “The CBO estimate released last night finally sheds light on the smoke and mirrors game the majority has been playing with the cost of their health care reform proposal. Over the first 10 years, this legislation builds in gross new spending of $1.7 trillion – and most of the new spending doesn’t even start until 2014. Once that spending is fully phased in, the House Democratic bill rings up at more than $3 trillion over ten years.
“Additionally, this bill cuts critical Medicare and Medicaid funding by $628 billion, accounts for nearly $1.2 trillion in tax and fee increases and will explode the scope of government by putting the nation’s health care system in the hands of Washington bureaucrats. The $3 trillion price tag defies common sense – we simply cannot add all this new spending to the government rolls and claim to control the deficit.
“If we continue to pile more and more debt on the next generation, they will never be able to get out from under it. The health care system needs reform, but this massive expansion of government, financed by our children and grandchildren, is the wrong way to proceed.”
And listen…this is what our government believes will be the cost. But look at programs our government has run historically and you find decades of added costs and overruns that our forced onto the taxpayer.
Insanity

See author page

More from the Catholic Bishops on healthcare, of which I agree completely.
Larry I wonder ( I ask this seriously, not in sarcasm), how “smart” you will continue to think the Catholic Bishops are when they up the Senate debate to include the protection of ALL human life? I suspect you will say, “We can add that other life stuff later”, which, BTW, would NEVER get added once the train has left the station.
I do have to agree with you that what the Bishops did was “interesting” and perhaps more brilliant than I had first given them credit. It appears that had they not put pressure on the dems, the bill may never have gotten out of the house, probably not. On first thought, that was a mistake, as in “Why didn’t you just KILL THE Bill (let it die)?” Initially, I was upset by this, knowing that there is no chance a final bill will be signed WITHOUT abortion, so why didn’t they just leave well enough alone and let it die in the house?
Perhaps they did out smart Pelosi. They HAD to have known she was playing them, but were THEY playing her? If so, it appears their ‘strategy’ (I use that word cautiously owing to the fact that faithful Catholic Bishops are first and always faithful to the teachings of Christ, not politics) was to get abortion first, and go for the rest of the life issues in the final bill. Thanks to Sarah Palin coining “death panels”, I suspect they will have the support of the majority of Americans behind them, since by logic alone, rationing HAS to occur in this monster of a bill.
I continue to predict that there is no chance a bill with “life provisions” (including non coverage of abortion) will EVER get passed under this Senate and President Obama. And that will be a good thing, because as the Bishops rightfully acknowledge, the rest of the bill, especially the economic issues, is far too complex. Consequently, I have now come to appreciate the Bishops’ fight, but they will need to save it for a less radical congress and less “agenda driven” bill.
I suspect all conservatives and most of Americans want improved health coverage, but not at ‘all costs’, especially at economic ruin to America and without the protection of all human life. Cardinal George, the leader of the US Catholic Bishops perfectly stated what I considered to be the epitome of what “Obamacare” despertly lacks:
@MataHarley said: ” Hang, the time I took here, I coulda done a post! “
Absolutely. You could have written a post which reached thousands but instead got diverted into putting all that time and effort into a personal exchange with one lefty. One wonders if maybe that wasn’t Larry’s goal all along: keep you from posting.
Confound his plan by posting anyway.
@PDill:
Your chosen quote is so important that I’d like to play it again:
I don’t see anything in it about “upping the ante,” on anything other than, perhaps, extension of benefits to the “illegals,” so that they are “treated fairly and not lose the health care coverage that they now have.”
You see the line which talks about protecting those at the “end of life,” and this triggers images of Sarah Palin’s outrageous “death panels.” I know that you believe another of Obama’s wet dreams is to be Grim Reaper-in-Chief, but that’s the mother of all hysterical scaremongering (and never has that phrase been more justifiably applied). I see nothing in the Bishop’s statement which indicates that they are going after anti-“death panel” language in the bill, where death panels refers to the so-called rationing of care. Maybe language barring the use of federal funds for euthanasia, which is a moot point, since no one is promoting euthanasia and no one is promoting assisted suicide or any such thing.
I am absolutely certain that the Bishops would have no objection whatsoever to end of life counseling, which is also moot, because Sarah Palin took that off the table, which is a great tragedy for cancer patients and many others. I again want to recommend Chapter Two in “Super Freakonomics,” where they talk about the limitations of cancer chemotherapy.
When you say “rationing has to occur,” I agree with you. Rationing is already occurring. I don’t know if you saw that article from Health Affairs which I quoted earlier (#55). Let me quote it again:
http://content.healthaffairs.org/cgi/reprint/13/4/22.pdf
Here’s what no one around here can seem to get through their thick skulls: We already have rationing. Let’s look at people who don’t have insurance. I had a fraternity brother named Gary, who was self-employed as a printer. The business was good enough that he could pay for his apartment, and clothes, and food, and car, and very modest entertainment needs. But he also had to moonlight as (of all things) a funeral director. One day, out of the blue, at age 59, he developed chest pain. It ended up not being a heart attack, but rather a very strange type of cancer, invading the sack (pericardium) around his heart.
Now Gary didn’t have health insurance. It would have been a major financial strain to buy health insurance; in addition to Gary not having a lot of money, he was a mild diabetic, which made him virtually uninsurable. You might fault Gary for not getting some type of insurance anyway, but he didn’t. Now, if Gary had insurance, he’d have been treated with chemotherapy right away. In point of fact, some of the tumor from his diagnostic biopsy procedure was sent to our lab. We ran our tests for free and found two drugs which looked extremely active against Gary’s tumor. Although I did, indeed, “diss” chemotherapy in my quoting “Super Freakonomics,” what I was referring to, end of life wise, was the situation where the patient has already received chemotherapy and perhaps the tumor shrank or even disappeared, at one point, but which then finally came back for good. My sister has been battling ovarian cancer for more than 6 years; she’s had multiple remissions and multiple recurrences. But, with many patients, there comes a point where it’s obvious that it’s not working anymore and that further treatment will just make the patient feel much worse and won’t help them live longer. It is at these points that end of life counseling is required. Because of Palin, it won’t be given and oncologists will just get richer, pushing more chemo — but I digress.
Getting back to Gary, he was newly-diagnosed and had never been treated with even a single dose of chemotherapy. He might have been one of those patients who had a truly dramatic response and remission, and he might still be alive today, more than 4 months later, and he might still have been alive next year. Our tests indicated that he’d have had a very good chance of responding to two of the entirely “standard” chemotherapy drugs. If he’d had insurance, he’d have been treated within a week from his diagnosis. Instead, the oncologist who was on hospital call for now emergency patients and who became his doctor and therefore couldn’t just abandon him instead simply scheduled Gary’s follow-up appointment for evaluation for chemotherapy for ONE MONTH AFTER HIS HOSPITAL DISCHARGE. Gary didn’t have insurance. He only had Medi-CAL. Medi-CAL doesn’t pay squat for chemotherapy (unlike Medicare, which pays very well). The doctor would have lost money treating Gary; so he didn’t.
And Gary had to be re-admitted to the hospital 3 weeks after his hospital discharge, from complications of progressive cancer. He died several days later, never having been treated once for his cancer. This would never have happened, if he’d had insurance.
This type of thing goes on all the time in America, for people without health insurance. Gary was not an irresponsible person. He didn’t deserve what happened to him. He was, quite literally, rationed to death. People without health insurance are rationed to death in this country all the time. These are the “Tier 1” patients referred to in my cited article. What about the “Tier 2” patients, which are typical people with average insurance? They get rationed, also, only not as overtly. They get rationed with respect to choice of doctors, choice of hospitals, choice of drugs on the approved health plan formulary. They get rationed with respect to treatments, although they don’t know it. Their doctors are experts on what their plans pay for and what they do not. So they only receive treatments which are covered under their health care plans.
Some health care plans are very generous with respect to hospital benefits. Patients with these policies stay in the hospital longer, while patients with health care plans mandating short stays are booted out, often literally with their surgical drains still dangling. Most people have heard about the in and out child deliveries and in and out surgeries. People with the best insurance (what I might call concierge insurance) don’t have to go the in and out route. The rest are rationed to in and out. There’s lots and lots of rationing which goes on everyday. Not decided by government “death panels” (truly the most vile political scaremongering I’ve ever heard; and Sarah Palin has directly contributed to the pain and suffering of hundreds of thousands of future cancer patients, and I consider her to be an utterly despicable, self serving human being); instead decided by health insurance operatives.
When people speak of the horror of rationing, they have no compassion whatsoever for the people without health insurance, who are literally being rationed to death every day. They are speaking about rationing for THEMSELVES. Well, most of those people are already being rationed. If they don’t want to be rationed, they have the option of purchasing concierge level insurance or paying out of pocket. They’ll still have that option under Pelosicare.
I noted earlier that some forms of chemotherapy currently cost $10,000 per month and one year’s worth of treatment has to be given to extend life by one month. $120,000 for one month. Without unlimited money, is there a point where cost effectiveness has to be considered? What about future drugs, which may cost $20,000 per month? This is not fanciful; it’s here today. I frequently do tests on tumors where I come up with the best drugs being Avastin plus Sutent. The cost of giving both of these drugs together can be $20,000 per month. No insurance will currently pay for this. Some of my patients do receive treatments like this. How? They pay for it out of pocket (not to me; I don’t treat the patients I test, because I’d consider it to be an enormous conflict of interest to do so).
I keep pointing out that health insurance premiums for small businesses like mine are going up 15% this year, after doubling during 8 years of President Bush. What I’m saying is that rationing is already here, and it’s going to be worse. Who do I want doing the rationing? Certainly not Wellpoint Blue Cross, behind closed doors. I want coverage decisions made right out in the open, as it is with Medicare. With public announcements in advance of hearings. Opportunities for all to weigh in, provide data, speak at open public hearings, public deliberations by panels of outside experts. Posting of provisional recommendations. More opportunity for public comments and political pressures by Congress. etc. etc. These are the so-called “death panels.” The insurance industry has them. They are private, closed doors affairs. Medicare has them. They are transparent. Pelosicare will certainly have them. That’s the way government works. Transparent.
Interesting article in the news yesterday. Cedars Sinai Hospital in Beverly Hills — hospital to the rich and famous — seems that they horribly overdosed 260 patients with radiation during CT scans:
http://www.latimes.com/news/local/la-me-cedars10-2009nov10,0,2052232.story?track=rss
What was unusual about this story is simply that the mistake became public knowledge. Probably, it was too big to cover up. If this had happened in a VA hospital, the outcry would have been deafening. Private hospitals and private doctors aren’t under the same conditions of transparency as are public institutions and public employees. Private sector medicine typically is allowed to bury its mistakes in private.
In short, I trust public institutions to make “rationing” decisions much more than I trust private institutions. Since I don’t want to be rationed, I’ll keep cash reserves to pay out of pocket and I’ll have the best supplemental insurance I can obtain. But I want basic care, with no lifetime payment limitations, to be available to everyone, like my friend Gary.
I love what the Catholic Bishops are doing. They are working for medical coverage for all, as they have been doing for decades. They are working to actually reduce abortions, which is what will happen if Pelosicare gets signed into law. They are working for a conscience clause, which I also support. It looks like they will also be working to extend coverage to “illegals,” from the language of pdill quotation (above). They are working to get the best deal they can. If they don’t get 100% of everything, I’m sure that they won’t walk away from the whole thing (as the GOP has done) and get nothing. They’ll do the best that they can and ultimately take what they can get.
I ask you again, pdill, do you support what the Bishops are doing? In the end, will you support Pelosicare (or whatever version of it finally gets signed into law) if the Bishops end up supporting it?
I’m on the side of the Bishops. I support them 100%. I think that the Bishops actually helped Pelosicare get through the House. This gave the Democratic moderates “cover” to vote for the bill. I think that this will have the same effect in the Senate. Senators voting for the bill can claim that they are on the side of the angels, which is exactly how I look at the Bishops.
Coverage for all Americans. Yes! Reduce abortions — actually reduce abortions and not just spend another decade paying lip service to overturning Roe v Wade — yes! Conscience clause — yes! Coverage decisions made transparently (I added this one) — yes, yes, yes!
– Larry Weisenthal/Huntington Beach, CA
@Mike.
I love Mata’s postings. Frankly, without her participation here, I’d find another blog. I always learn a tremendous amount by reading them and I enjoy debating her.
– Larry W/HB
@openid.aol.com: Yes, I am sure it strokes your ego immensely to have Mata devote so much time to debunking your leftward lunacy. And I don’t fault her for doing so except to the extent that it keeps her from devoting the time necessary to reach the wider audience.
Now, if you two want to get a room somewhere and hash it out, fine by me.
@Mike: Here’s what’s special about Mata. She actually writes original stuff. Flopping Aces is mostly a clearing house for links to news stories, videos, op-eds written by others, etc. With brief comments appended, which are typically just a hearty “hear hear.” Curt does do a very good job of scanning the internet for fast breaking stories, videos, op-eds, etc. It’s a valuable resource for that.
But, with respect to original writing. Original thinking. Original analysis. Well, let’s say that this is a might thin. Once you get beyond the war on terrorism and national defense, where there is some seriously original thinking here. But back to Mata. The best of her blogposts are some of the best conservative blogposts I’ve ever read. As opposed to simply taking a single weblink, posting an excerpt, and making a comment about it, she strings together a narrative, based on a common theme, incorporating a number of different internet sources and links, and puts it all together to make a unified story, supplemented with a lot of thoughtful writing. No one does this as well as she does. I’ve got another family member and a friend surveying FA, and they both agree with me. Mata is the best.
The other thing about Mata is that it’s possible to have an actual debate with her, on substantive issues, devoid of an hominem, personal attacks. This is not to say that she doesn’t have some very sharp claws, that she’s not at all shy at using to inflict great bodily harm, when she gets her dander up, which always happens when she starts to shred my own comments, but the emphasis is on destroying the argument, as opposed to destroying the person. There’s a big difference between the two.
– Larry Weisenthal/Huntington Beach, CA
Always amuses me when people think blogs are something they are not. They are not magazines with professional writers who write original content. They are, as you describe, brief snippets of the news of the day from the blog owners perspective. That’s it….nothing fancy. FA is lucky enough to have some great writers who do write original content sometimes but that is time consuming and with all of us having day jobs its not going to be a common occurrence
@openid.aol.com:
A few questions:
First, you state that Gary’s doc chose to deny treatment because there was no insurance coverage. Doesn’t this violate the Hippocratic Oath or ethical standards that the doc swore to uphold? If so, did you report the doc? If not, why not?
Second, Gary was a friend of yours. Obviously you thought enough of him to perform the lab tests free of charge. Did you also extend to Gary the option of free chemo through your facility? If not, why not? You do, after all, by your own admission enjoy an obscene 20% profit from what you do day in and day out.
Frankly, the story about the doc choosing not to treat Gary due to lack of insurance doesn’t smell exactly right.
Your friend Gary chose to not have health insurance. He exercised his God given right of freedom of choice and, ultimately, suffered the consequences of that decision.
To #109 – And that is the hallmark of a good blog – Curt jumpstarts the discussion – and the commenters weigh in – with experience, knowledge, original thinking, clear-headed analysis, informed and informative points that help us all as we go out to have these arguments in our own community, in our own circle of friends.
It’s how honest discussions happen, and how people get the facts that the reporters either don’t know or won’t report.
Larry I’ve always made it clear that I’m for reformed health care providing it protects all human life and isn’t lining the pockets of the “caretakers” at the expense of patient care. I DO support the Bishops fight for life, and made it clear in my last post that they are bishops not politicians, trying as much as possible to “get GOOD healthcare” but to also keep the “doctor of death” OUT of what’s on the table.
My goodness, even my favorite atheist/liberal/democrat writer, Camille Paglia, gets it right on healthcare, along the lines of what most of us at FA have been saying all along; keep it fair, simple, and use COMMON SENSE. Why we are demolishing the house and ‘rebuilding’ because of a ‘leaky faucet’ is the first sign that this isn’t about ‘health care’. We could have already insured all of the “Gary’s” who are uninsurable with the money we wasted on the scam “stimulus” or H1N1 hype “national emergency”, an ‘emergency’ so terrible the Obama girls didn’t even get the vaccine. How about we get what “THEY” get Larry, they being the elected in Washington?
Excerpt from today’s Paglia column
As for Palin, you sure make a bold leap to “drug resistant chemotherapy.” How about the 2o year old who ends up a quad as a result of an auto accident, or the overweight teenager or middle aged mother of two who needs expensive (and available), life saving treatments? That’s the kind of stuff that has everyone with a conscience concerned. I can assured you that under O’care, there simply won’t be enough docs to be pumping drug resistant chemo into the newly diagnosed, being that most of them won’t live through the 6 month or more waiting list! In addition to the disabled or the “worthless to society crowd because they can’t control their eating habits or didn’t get a college degree”, Palin is also referring to the mentally challenged. Shame on you Larry for making the case for Palin killing cancer patients when in fact, she will have greatly contributed to the salvation of the “non elite” crowd.
I don’t disagree with you that insurance companies ration, but it also works the other way. I once had an internist BEG me to have a bone density test (I was 30 years old). I told him flat out no and he at least was honest and told me I had good insurance that would pay for it (he had just gotten his “new bone density scanner). That’s just one example of many, but with “insurance rationing” also comes “physician abuse.”
I also don’t disagree with you that the private insurance payments are absurd and only getting worse. I currently live between two coasts of the country because I can’t take my “Blue Shield” out of CA. Ok, I admit I still love CA in the winter months, but if it weren’t for health insurance, I would NOT continue to be a CA resident. My policy just went up another $200 a year, in the middle of the year, and that’s for high deductable.
Bottom line, and to put a rest to your question “ Do I agree with the Bishops”, it’s hard to answer directly. I certainly believe in their fight for human life, and you too agree with the conscience clause which I respect. Unlike you, I KNOW they will not compromise without the conscience clause, because doing so would mean every Catholic Hospital in America will have to close. I also know, based on church teachings, that they are against socialism and big government control.
The reality is, and we will know soon enough (feel free to bookmark this page), there is no way healthcare under Obama will pass with the “life” issues demanded by the Bishops. That’s because, as I and many have tried to tell you, this isn’t about “healthcare”; it’s about single payer power.
There will be no Obamacare, and that will be a good thing. Hopefully, after 2010, we will get a fresh, non-corrupt, and “educated” new congress (both parties), and pass a simple bill, starting with one that allows insurance to cross state lines and be competitive.
If in the end the Catholic Bishops end up being the “deal breakers” for Obamacare, then hey, maybe God is looking out for us.
As for as Mata and Larry, I agree political debate doesn’t get much better. I’ve written about it here before, the epitome of liberal/conservative debate; erudite, respectful, but with the needed jugular; no wimps here!
If only Larry could be Mata, wow, would love to read “Larry as a conservative.” For now, until hell freezes over, I’ll just enjoy the debate(s).
Rose (#111), I agree with you too. Orignial writing is always great when the talent and time is there, but that’s not to say that some great insight isn’t often gained in the “ripped from the headline” discussions. Larry I think you are wrong to sell it short. Even if this is a conservative blog, we get plenty who don’t line up with a yes yes yes.
Mata and Larry: CNN could use the ratings; should hire you two. Even better, you two would make a killer Sunday show!
@Aye (#110): Very reasonable questions you ask. I’ll reply in detail, but not until after 6 PM PST today. Also, I really haven’t forgotten about Missy’s entirely excellent points on the issue of why the GOP didn’t reform health care, when they ostensibly had the chance. Thanks for asking; I’d like to talk more about my friend Gary.
– Larry W/HB
@openid.aol.com/runnswim:
You’re right Larry.
This is a perfect example of you trying to have it both ways.
You go on and on about how the Bishops have pulled off some sort of coup and that their accomplishment represents a watershed moment that will reduce the number of abortions.
However, in order for that contention to be true you would have to admit that there will be a massive migration onto the public option, forced or otherwise.
Yet you’ve spent the greater majority of your interchanges on this thread claiming that there will be no such mass migration and that the public option will only affect a minor number of people.
So, which is it?
Of course none of that really matters because it is becoming more and more obvious, that even from the moment of passage, the non-abortion restrictions were destined to be stripped out.
@aye (#116):
No, I’m not trying to have it both ways. Here’s what I think:
Firstly, the abortion proscription applies not only to the public option but also to the private insurance pool, which will be established for the benefit of small businesses (like my own) and for individuals without employer-provided health insurance. All the plans in the private insurance pool, in addition to the public option, will be prohibited from paying for abortions, whether or not a given purchaser pays entirely with his/her own money or has the purchase partially subsidized with government funds.
Now, the issue is this: How many people will be covered by either the public option or by the insurance pool (“exchanges”)? Mata seems to feel as if virtually everyone will be covered by the public option — that the public option will out-compete private insurance plans, owing to government-related unfair competition advantages. I tend to agree with Mata — although this will take a very long time — long after Obama, Emmanuel, Frank, Sibelius, et al have left the scene. The article you cited stated that the anti-abortion provision would have a rather small impact, because there would be relatively few people in either public plan or insurance pool. This is what the Democrats have been claiming. They claim, for the vast majority of people, that the status quo would be maintained (“if you like your present insurance, you can keep it.”). I just thought that it was amusing that you cited and linked an article which totally agreed with the Democratic position and totally disagreed with Mata’s position. Not a big deal, just a little bit of a “gotcha.”
My personal prediction is that, from the beginning, there will be at least several million people who go the route of either the insurance pool or the public option. Since half of these will be women and since many (such as, for example, small businesses currently paying lots of money who want to change to a more affordable plan) will be switching from private policies (which cover abortions) to the insurance exchanges or public option, which don’t cover abortions, the total number of abortions would then go down — not to zero, but they’d definitely go down.
Right now, I’m predicting that the Stupak Amendment will remain in the final bill signed into law by Obama. I think that there’s about an 80% chance of this, actually.
– Larry Weisenthal/Huntington Beach, CA (P.S. more on Gary later on)
GASP! LOL
And yes, my projections are long term, and not immediate. So yes… we are in agreement. Our disagreement lies in that this is good in your opinion, and I believe it to be a fiscal nightmare that will sink the economy.
@aye # 110
Excellent question. Doctors deny treatment every day for financial reasons. Treatment decisions aren’t always black and white. Let’s say that you have coronary artery disease. This can be managed either “medically” (with lifestyle changes, anticholesterol meds, etc.) or it can be managed with angioplasty or it can be managed with coronary artery bypass surgery. The literature is not clear, in most cases, which is the best approach, particularly for individual patients.
Now, my friend Gary was a mild diabetic. Let’s say that he had heart disease and not cancer. And he didn’t have insurance. To which one of the three doors do you think Gary would be directed? Pills? Angioplasty? Bypass surgery? Let’s say that he had great insurance. Which door then? Would it have mattered if he’d been referred by a family practice gatekeeper to an interventional cardiologist (one who does angioplasties himself) or to a non-interventional cardiologist (who doesn’t have a financial stake in whether the patient gets pills or angioplasty or bypass surgery?
Let’s take prostate cancer. No definitive evidence that primary treatment makes any difference at all. Could be managed by “watchful waiting” vs external beam radiation versus implant brachytherapy versus open radical prostatectomy versus prostatectomy using a Da Vinci robotic machine. I can tell you that 95% of the decisions on what to offer the patient are based on economic considerations. No insurance versus insurance. Whether a therapeutic radiologist or urologist first gets his hands on the patient. Whether or not the urologist has invested in a DaVinci robotic machine.
Pdill gave a very typical example of this: she had good insurance, insurance pays for procedures and not for counseling (e.g end of life counseling or any other counseling), doctor in question has a brand new expensive machine that he needs to pay off before he can start making money off of it.
This is why the US healthcare system fails as a capitalistic economic model. In a market economy the purchaser wants to keep the purchase price down, the seller wants to keep the price up and the price seeks its own level. In health care the sellers (doctors) are the ones who make the purchase decisions. Any doctor worth his salt can talk a patient into doing anything the doctor wants the patient to do — at least 90% of the time, anyway.
All the incentives in the US healthcare system are to do procedures in patients with good insurance and do the minimum possible for people without insurance. So people with good insurance get way too much treatment and tests and people without insurance don’t get enough treatment and tests.
Now, why didn’t I “report the doc?” For what? The last time I talked to Gary, he was still in the hospital the first time. I told him, whatever he did, he HAD to be seen by an oncologist in the hospital before they discharged him, because otherwise he’d never find an oncologist on the outside who’d agree to assume his care, given that he didn’t have insurance. So he was seen and that doctor ended up “stuck” with him. I told Gary to call me, if he had any problems, after his discharge. The next time I heard from him was three weeks later. It was then he told me that the oncologist had still not seen him following hospital discharge and that he was having trouble breathing. He went in the hospital the same day. My brother (who lives in South Orange County, down near where the hospital was located) went to see Gary. He looked very bad, according to my brother. At this point, Gary (under the care of a hospitalist, after admission) was seen by his oncologist. The oncologist told him that he was too sick to receive chemotherapy, and that he (the oncologist) would advise against it. I’d probably have agreed with this, at this point. The next day, Gary died.
Now, why didn’t I “report” it? For one thing, this sort of thing is very typical. When oncologists treat patients without insurance, it’s not just their time that they are donating. They have to buy the drugs themselves. When the patients don’t have insurance, it’s the oncologists who have to pay for the drugs. Medi-Cal doesn’t begin to pay for the costs. So people without insurance don’t get nearly as much chemotherapy as people with insurance, just as people without insurance get a whole lot less surgery. For reasons which have very much to do with economic advantage or disadvantage to the doctor.
So the doctor just says, look, he looked OK when he left the hospital. I gave him a follow up appointment (true, only 4 weeks down the road after hospital discharge, during which time the cancer progressed to a point where the patient couldn’t tolerate chemotherapy).
Now, if you heard this anecdote and it happened in Canada, you’d go on a rant about socialized medicine. But this thing happens all the time in the USA. You pay cash, at time of service (as I do, for most medical services, as I’ve got $8,000 deductible insurance) or else if you’ve got really great insurance, and the waters part for you. You’ve got a standard Blue Cross PPO policy which squeezes the doctor and your appointment is next week or in two or three weeks and you get the sorts of tests, surgery, and drugs which miraculously match your insurance benefits perfectly, so you are so pleased with everything, even if what you are getting may be different from that which someone with really good insurance is getting. And if you don’t have insurance — well, then you are Gary.
As I noted, I don’t treat patients myself. I made the choice, 17 years ago, to devote my career 100% to developing and providing my testing services for cancer patients. I consider it an unacceptable conflict of interest to both perform tests and treat patients. Oncologists make lots of money giving chemotherapy — Super Freakonomics says that they make over 50% of their income from giving chemotherapy (i.e. being retail pharmacists, as opposed to being doctors). Some forms of chemotherapy are very lucrative. Other forms of chemotherapy make no profit whatsoever. In the real world, chemotherapy decisions are very often made on the basis of which drugs make the most money for the oncologist. This has been documented in peer review research. Since the crux of my service is to come up with a specific treatment for a patient, there would be the temptation to emphasize certain findings over others to justify more lucrative treatments, were I involved in this. Since I’m not involved, I can do what’s best for the patient, as whatever I recommend won’t influence my income whatsoever. So I wasn’t in a position to treat Gary myself.
Not really. I’m a sole proprietorship, not a corporation. That 20% profit represents what would otherwise be my salary. In a corporation, the corporate officers get a salary and this is included in expenses. Profit is what remains after expenses. In a proprietorship, the profit IS the salary. And my profit/salary is not, I assure you, in any way out of line. The only thing embarrassing with my tax returns have been my recent comparative stinginess with charitable donations; but this is because I’ve had to pay for putting two kids through private colleges, which I’ve financed, in part, with a second mortgage on our home. I do pretty well, but there’s nothing at all obscene about the money I make, relative to the work I do.
I’ll go further than that. It stinks. But it’s 100% true.
Gary didn’t “choose” to be a diabetic and to be 59 years old and to be self-employed (as a printer, moonlighting as an $11 per hour funeral director) in the middle of a recession.
This goes to the heart of the difference between being a conservative and being a liberal, I guess. I’m not claiming any moral high ground. I understand the advantages of small government and economic Darwinism. I just happen to think that the US health care system sucks and I’ve been all over a large part of the economically-developed world and know doctors in all these countries and I happen to think that they’ve got much better systems than we’ve got. I want a system which is much more like theirs. So it’s just an honest difference of opinion.
– Larry Weisenthal/Huntington Beach, CA
Larry I agree with what much of what you wrote to Aye, as it is on track with the point I was also trying to make. While our current system “under treats” the uninsured, it just as much “over treats” the well-insured.
Do you understand that most of us against Obamacare are NOT in love with the status quo, we only prefer it over the train wreck that is about to happen if we don’t stop it. I also think it is fair to say that none of us, and I would suspect you included, have any problem with the standard of medicine in the US, only the execution of it.
What we need is INSURANCE REFORM, not “health reform.” So here is my burning question to you. Why aren’t you on the bandwagon to change what matters most, competition between states for medical insurance. If my memory is correct, Mata made mention (somewhere recently) that she thinks the reason relates to states’ rights. I don’t think it has as much to do with the rights of each state as it does the monopoly and kickback of each state, and to both parties.
The “solution” is so simple and logical to just let the “free market” work; consequently all of America can be insured as one big “group” at an affordable cost. The fact that this isn’t even on the table should be more than enough evidence that this is not about insurance, only a power grab. Would you please answer my question as to why you prefer a monster national bankrupting government bureaucracy, with everything from “dog insurance (I kid you not), to grant monies for minority nursing students (?), to prison sentences for those of us who don’t pay up?
On another note, I want to revisit your outrageous attack on Sarah Palin yesterday claiming that she has “undone” the ‘counseling’ treatment of cancer patients (like anyone is even going to be alive to need it after the “waiting period” if Obama gets his way). Despite that fact that she was referring more to the disabled (young and old), here’s proof that you are dead wrong on that. This may shock you Larry, but the “panel”, has already been put into place via the “stimulus package.” Here’s an excerpt but you might want to read the whole thing, as it will prepare you for a soft landing as you continue to live in your Obama fantasy world.
As for Gary, that’s a very heart-wrenching story. None of us can bring Gary back, but I bet if he was here, and was given a choice of affordable private insurance vs. Obamcare, it would be a no brainer for this simple reason: If Gary couldn’t afford private insurance, he certainly wouldn’t be able to afford Obamacare, as will be the case with most of us, even those of us who “do pretty well.”
If we ever get the monopoly broken on the state to state issue, the rest will fall into place. Docs will make the wages they justly deserve without having to be MBA’s and salesmen, patients will get lifesaving care they need, and the US will continue to be the best place in the world for medical treatment.
@PDill: The American Thinker article has no relevance whatsoever to the now scuttled (thanks to that egotistical monster Sarah Palin, who has single handedly condemned tens of thousands of cancer patients to being poisoned with chemotherapy in their last days, to the great advantage of oncologists, who now have every incentive to simply keep pushing poison, as opposed to sitting down and talking to the patient for 45 minutes to realistically explain the situation and all the alternatives).
Comparative effectiveness research (which I support, 100% and which every thinking American should support 100%) has nothing whatsoever to do with end of life counseling.
Why do we need comparative effectiveness research? Because we can’t pay for everything. Right now we have care being rationed by doctors on the basis of the patient’s insurance and the financial advantages to the doctor.
Is it comparatively effective to spend $120,000 to prolong the life of a cancer patient by one month? How about spending $240,00 to prolong life by one month? I have illustrated that these are not theoretical concerns; they are real world concerns today in an environment where the cost of private insurance premiums for small business is going up by 15% in this year alone, right in the middle of a recession with 10% unemployment. You don’t think this is as much a job killer as any tax of similar magnitude? What about quality of life? What’s the trade off between quality of life and quantity of life? Without comparative effectiveness research, we have no data on which to base the decisions which any fool can plainly see are going to have to be made.
These decisions are made every day, in completely opaque privacy, by insurance companies, and, just as much, by private practice doctors, who are very careful to perform what we in the profession are honest enough (among ourselves) to call a “wallet biopsy” before we even agree to evaluate a patient, and it is the results of the wallet biopsy which so often determines just how far we go with our tests and treatments — with favorable wallet biopsies, we perform more tests and provide more treatment than is in the patient’s best interests.
We are human beings and we are motivated by the same things which motivate anyone in a capitalist system — only we control both the selling and the buying. What we choose to sell is, to a considerable extent, influenced by the results of the wallet biopsy. This is rationing by insurance companies and rationing by doctors, who can do this, because there is little definitive comparative effectiveness research to shame them into making the best choices for the patient.
I have vastly greater trust in transparent public insurance than I have in opaque private insurance. You have some crazy notion of Obama and Emmanuel joyously getting each other off by deciding, in the privacy of West Wing offices, who’s living and who’s dying.
It’s hysterical scaremongering and it’s outrageous and it’s hurting sick old people (and often sick young people, as well) living in the real world of life, as opposed to in the fanciful world of conspiracy theories.
– Larry Weisenthal/Huntington Beach, CA
@openid.aol.com/runnswim said: “@Mike: Here’s what’s special about Mata. She actually writes original stuff. “
That kind of cheap shot is beneath you Larry. I’ll keep it in mind as I research my next original piece and see if you notice when I post it.
Clearly YOU have run out of anything original to say on this issue. You just keep repeating the same worn out talking points over and over and over as if they are true if you say them often enough.
Give it a rest. Obama’s takeover of health care if failing and your flailing won’t save it.
@Mike. I was cranky when I wrote that. I apologize. You are a true vexation to my spirit, but you do often take a lot of time to research and write thought provoking pieces. – Larry W/HB
@ openid.aol.com/runnswim (Larry)
Well, there it is. The whole reason for Larry’s liberal leanings. He needs government to step in to stop him from being greedy, because he can’t do it himself.
Are you serious. Sarah has nothing on your boy Obama. President Obama sent a video to the anniversary of the fall of the Berlin Wall. In his speech, did he mention the work of Reagan? Thatcher? Nope. He did find a way to work himself into the speech though.
I’m seriously tired of hearing this $120,000 a year to prolong life for another month. It doesn’t make sense. Mathematically speaking, if I was paying $10,000 a month for a drug that only kept me alive for another month, I’d probably skip the next 11 payments. Just saying. I’m not a doctor, but engineering requires maybe a little more math than you super smart doctor types.
I can’t speak for anyone else, but if (God forbid), I ended up with a terminal disease, I would speak to my doctor about everything, including end of life. However, since I trust most doctors about as far as I can throw them, I would take their advice with a grain of salt.
Leave the rest of us out of your healthcare utopia. Just because you and some of your colleagues can’t help yourselves from digging into patients with deep wallets, doesn’t mean everyone is that way. It’s mostly just liberals.
@Aqua (#124):
Thank you indeed for that — which gives me a splendid opportunity to make another point about the reality of medical care (hint: even mathematical genius engineers can’t make good decisions when the doctors who play them like violins — in our current basket case of a health care system — don’t tell it like it is). Like yesterday, it’s going to have to wait until after 6 PM PST.
– Larry Weisenthal/Huntington Beach, CA
Original larry? Take your own advice. As Mike pointed out, you keep saying the same things over and over. You even used the “echo chamber” complaint for about the 3rd or fourth time that I can recall. You should have been here for the Newt Gingrich/NY-23 debate.
You are very much a liberal. You have no insight into yourself, live in extreme denial, and project onto others your own short comings.
Boyo… it’s taking some time to load this mondo thread of yours, Curt…. LOL
And I see I’ve some catching up to do in the plethora of related subjects here. But first, thanks for the kinds words directed my way INRE both debate and posts. It is always nice to hear. But as @rose pointed out, the mixture of both original analysis and news stories with brief supporting commentary is a good thing because a blog, like FA, generally thrives and shines on it’s participants. Authors and guest posts throw out subjects to provoke stimulating conversation, and I can say the FA is abundant in just that.
First, INRE your friend Gary, Larry. Two thoughts immediately popped into my mind. One is that his cancer must have been very advanced to be terminal within three weeks.
LarryGary (sorry) is not much different that most of us sole proprietors and/or independent contractors. Individual insurance, as you well know, is costly and has high deductibles. Which is why I advocate more “groups” be created. If any of us has a few associated “group” plans from which we, as individuals, can choose, the pre’existing condition (the lies constantly being spread by Pelosi and ilk) simply go away via federal statute. If Gary had a choice of “groups” to join for affordable coverage, perhaps he would have.But then, as you say, times are tough for the sole entrepreneur. It’s hard to obligate to an additional $300+ a month for health insurance. Sometimes biz is good and it’s no problem. Other times it’s a choice between that $300+ health insurance premium or paying your mortgage. If you don’t pay it, you get cancelled.
The bizarre reality is that isn’t going away with any mandated public option. The only difference is Gary would have been required to purchase health insurance, or face IRS financial penalty and/or jail time. How, pray tell, does that improve Gary’s reality? If you can’t afford health care… perhaps even if you qualify for a group… how is “mandating” you pay for a public option health care going to change that reality? Especially since with the increased taxes, there will be even less earning power for the Gary’s of the world.
The second thought about Gary’s end days was that he did indeed get his appointment, thanks to your counseling on how to get around the rules and the doctor’s “wallet” attitude. Kudos to you. But why complain about an appointment a month away? As you say, this is no different than those with poor coverage, and is probably months ahead of social health plans in Canada, England. Were Gary in either of those countries, and his cancer as advanced as it seems to have been, the result of his death would remain the same.
So I fail to get your point, Larry. Uninsured Gary was getting care, and about the same quality of care and service he’d get under a public option. The difference is, Gary didn’t pay out thousands a year for the same poor service. In one way, he was ahead of the game.
To dash to the point, not once in your story of your friend did I see any improvement for his scenario had O’healthcare been in place, Larry. Fact is, he was seen and he did get care…. about the same kind of care you find in social health programs which O’healthcare is emulating.
Now we come to your emotional tirades about Palin and end-of-life counseling. I have no idea where you come to the conclusions you do, and your obvious hatred for Sarah, but I suggest you need to re’evaluate you… or any medical professional’s…. import and place in an individual’s life.
To use O’s favorite phrase, “let me be clear”… who the hell annointed you or any medical professional the official care taker of end of life issues? And exactly why would you want to see them mandated, which then can be tied to receiving medical care? (i.e. you *will* take end of counseling treatment or you will not get the meds you need… )
If I were told I was terminal, and the doctor decided to put an expiration date on my forehead (none of which I believe, BTW), that doctor or any doctors is the last individual I need for end of life counseling. Yes, there are therapist services for this. But should they be mandatory when you have family members, clergy, funeral services, estate attorneys etal… all whom help plan end of life issues? What is this demand for guarantee insurance “payment” for end of life services you’re fixated on when there are considerable other options?
What I expect from medical professionals is that they give me the alternative treatments (or not) for any illness I have. They may wish to give me my death date, but frankly I’ll take that with a grain of salt. Short of that, I don’t need no end of life counseling from the medical world. Wrapping up my affairs has nothing to do with the medical provider. It has to do with property estates, and perhaps even a “bucket list”. (love that movie….)
But then, I’m no fan of psychiatrists and therapists. Most I’ve met are more loopy then the average stressed out citizen, living in their own lives of disarray. That’s my own personal opinion. But I also don’t think a psychiatrist, or any member of the AMA or medical professional is the end all/be all quintessential “end of life counselor”. And to mandate any counseling is, IMHO, nothing but a scam to withhold benefits.
So your blame of Sarah, to me, strikes me as purely emotional, and founded entirely on your notion that your medical colleages are the “gods” of end of life counseling, and cannot be replaced by anyone else who just may provide the same graciously for free out of love and responsibility.
@mata: Will have to wait until tonight for in depth response, but can’t let one thing go by until then:
It’s a straw man argument. I never said that, thought that, felt that. Quite the contrary: the whole point of end of life counseling is to spend a lot of time with the patient, carefully explaining the reality of the situation, and allowing the patient to make an informed choice.
Larry, I appreciate your clarification. However you are speaking from a medical providers’ viewpoint, and seem to place more emphasis on their per-hour services than the alternatives that cost nothing.
As you say, the medical providers duty ends when he explains the reality of the situation, and allows the patient to make an informed choice. This requires “per hour” services that are labeled “end of life counseling”? When a doctor comes in with a prognosis, does he/she patiently explain the medical options or not… sans any extra charges? At that point, consider the patient “informed” enough to make their decision.
However I see no reason why the patient must then be referred to a professional “end of life counselor” who charges by the hour when they can go directly to their estate attorneys, their family or their church. Even the destitute can obtain end of life services from any clergy or Salvation Army location for free.
End of life counseling, itself, is a straw man, IMHO. There is absolutely no earthly reason why it should be a mandate. It should be free advice, and hand the patient a list of free services and professionals that can provide aid at that time in your life.
@openid.aol.com/runnswim:
@MataHarley:
I hear Red Roof Inns is offering a holiday special on rooms 🙂
@Mata (brief reply; will respond in more depth later tonight): People have this vision of old geezers with Alzheimer’s being euthanized by death panels. The reality is the number one situation where end of life counseling is required is in “terminal” cancer. The oncologist has two ways to go on this: (1) realizing that people want to live and that they feel that the way to live is to receive treatment and that, in metastatic cancer the only potentially effective treatment is chemotherapy, the path of least resistance is to just keep giving the patient poisons, while collecting revenue (and often big revenue) in the process. This requires about 3 minutes of explaining (oncologists don’t get paid for explaining, just for evaluating and treating). (2) realizing that there comes a point where chemotherapy is much more likely to cause harm and actually hasten death, rather than prolonging it, sit down with the patient, for 45 minutes to an hour and gently explain the reality of the situation, go over all the options, including non-chemotherapy options and hospice options, provide the patients with all the facts, answer all the questions and allow the patient to make an informed choice, which will often be to eschew further chemotherapy, which means that the oncologist won’t be making any more money off this patient, and, to top it off, the oncologist won’t get paid a penny for taking this extra hour to provide all of this end of life counseling to the patient.
Because of the heroic efforts of Sarah Palin to raise her own national profile by the most shameless scaremongering (that phrase again — take note, Hard Right, I am once again repeating myself, because it bears repeating, just as Mike and Aye think it bears repeating to keep posting the same Medicare cost overrun table and graph again and again and again and again) which I have observed since the Lyndon Johnson nuclear bomb daisy commercial, used against Barry Goldwater in 1964, — because of Ms. Palin, oncologists will be even more likely to completely avoid number (2), which requires time and personal stress (it’s unpleasant telling a dying patient that you’ve run out of treatments which are more likely to help than harm) and which costs you money and which you aren’t even paid for doing.
So tens of thousands of cancer patients are going to spend their last weeks and days being poisoned, rather than being comforted in quiet dignity, to satisfy Ms. Palin’s craving for adulation. That’s reality, not the fantasy of death panels euthanizing old people with Alzheimer’s.
– Larry Weisenthal/Huntington Beach, CA
@Mike (#130): I thought I had an invitation to stay with you.
Indian giver.
@openid.aol.com/runnswim: Remember this old Streisand/Diamond duet:
“You Don’t Bring Me Flowers Anymore”
I know you love Mata more than me!
Let’s just toss this one in there while I am at it:
Hey Mike, maybe you need to play “harder to get.” 🙂
Dang… had the reply half way done and lost my stuff… let’s try again.
Let me get this straight, Larry. What *you* consider “end of life counseling” is a doctor taking an extra 45 minutes to explain the risks/results involved with each treatment option? Odd… I consider that part of his job. For him not to explain is akin to me paying a guy to investigate a furnace system, then refusing to tell me the solutions without an extra charge.
Considering what you consider “end of life” counseling, I can see we’re having an apples/oranges debate about Sarah Palin. I’m relatively confident that were you to explain your version of “end of life” to her, she’d reasonably say… but of course a doctor should do that. It’s part of his job.
However that is *not* what Palin was addressing. So let me revert your train of thought to the original HR3200 Pelosi bill, pg 425 (which you can find in PDF version here.
This end of life counseling is a mandate for Medicare patients, called “Advanced Care Planning Consultation”, to be conducted by a physician, physician’s assistant or nurse practitioner who has State authority to sign orders for life sustaining treatments. The every five years (or more if some medical condition arises inbetween) came from the language:
This physician etal is supposed to be consulting with the Medicare participant about living wills, power of attorney, health care proxies, subsidary funding for advance care planning clearinghouses, and State legal service organizations, various state services and clearing houses, hospice, etal.
Did you catch that this was *mandatory* in that bill? And just why is a physician, physician’s assistant or nurse practitioner speaking to a patient about living will, powers of attorney, etc?
These services are available at no charge. To make them mandatory reeks of denial of medical services if you do not participate in such services that are available via many of the avenues I mentioned above, as well as state agencies.
Mandates are insidious, and unnessary. Don’t know how to say it any differently.
On another topic… dang… don’t want to interfere with a budding relationship between you and Mike. I wanna cyber divorce!
Just to clarify something, Larry…. you were speaking of the physician not being paid for his extra 45 minutes worth of time to ‘splain that chemo just may kill him faster than the cancer. This I understand well as I’ve lost four friends this year alone… dying by chemo and not the cancer.
The point is, the end of life counseling was for those covered by Medicare already, and just gave a larger staff of (IMHO) unqualified people to help patients plan for wrapping up their affairs. This is not the job of medical providers. It is their task… for the insured and uninsured whom they are treating… to explain their prognosis and the medical options available and under what circumstances. This costs them nothing but time… not the drug charges.
And it most certainly is out of the jurisdiction of the medical provider to be speaking of living wills and powers of attorney for their assets and heirs.
@ openid.aol.com/runnswim (Larry)
I look forward to it. I love a good math problem. Please put it in the standard form of:
ax² + bx + c = 0. Survivor is on tonight and I would like to knock it out before it starts.
Also, if I have a problem with my car, I will research that problem before I go to a mechanic to make sure I know from which I speak. I do the same before I go to the doc-doc. I don’t enjoy speaking from a place of ingnorance. I can assure you, I don’t believe there is a doc out there that could play me like a violin. I’m built more like a Cello.
@ mata:
1. Not mandatory
2. Reimburses doctors, not clerks
3. Covers any and all end of life counseling, not just the non-medical sorts of things enumerated. The purpose of putting in language like that wasn’t to mandate any particular type of counseling; or to limit it to any particular type of counseling; it was merely to illustrate that the counseling could be comprehensive – even extending to such practical considerations as living wills — very important to doctors, who are faced with the decision on whether or not to call a “code” for a cardiac arrest.
Currently, all of this clerical stuff gets explained by low level clerks — a great percentage of the time. The clerks can’t begin to explain what really goes on with a “code” — broken ribs and much other gore. These things are better explained by doctors. The bill didn’t mandate anything at all. It simply provided reimbursement to doctors who took the initiative to talk about such things and answer questions.
In practice, as I said, the most frequent time when true end of life counseling would come up would be when oncologists decide that further chemotherapy would be more likely to harm than help. You say that it’s the job description of an oncologist to take the 45 minutes to one hour (and it can easily be that long — or longer — if it is done properly) to break the news to the patient that medical science has about run out of treatment options. I don’t disagree, but i really wish that someone would tell that to lawyers and other professional consultants. Doctors are a human as anyone else; they are more likely to take the time to do it right if they get paid for it. 45 minutes out of a busy doctor’s day is a huge amount of time. Oncologists can be taking care of hundreds of patients at a time, many or most of whom will eventually require such counseling (a huge burden, collectively), and, because of Palin, will be much less likely to get it.
http://mediamatters.org/research/200907290047
Yes, I know Media Matters is a liberal-oriented web site, but this is a very nice, concise summary. If you find fault or error with what is summarized there, feel free to point out what it is that they have wrong.
– Larry Weisenthal/Huntington Beach, CA
1: Not “mandatory”? Excuse me, Larry. But are you telling me you equate Congressional bills/language as an advisory brochure? If it’s in legislation, signed by a POTUS, it’s called LAW.
2: “Reimburses doctors, not clerks”. I’m sorry. What part about “reimbursing” physicials, physicians assistants or nurses’ practitioners for MANDATORY/LAW REQUIRED living will/powers of attorney makes them acting as “end of life counsels” on matters far outside their jurisdiction is okay with you?
3: “Covers any and all end of life counseling”…. any why should any of this be MANDATORY LEGISLATIVE LAW, performed by people outside of their jurisdiction, be reimbursed and mandated by the US Congress?
I will remind you, this argument is about you slamming Palin about her vocal opposition to HR 3200. I have provided language about what she was speaking of. Yes… it was *mandatory*. Yes, it was *mandated* counseling provided by medical professionals that included legal assets and other estate issues that they are not equipped to cover.
Yet you say Palin was “crazy”?
I think you never read the legislation, Larry. You preferred to carry over your disdain for Palin, and make up the rest. She was correct. None of this should be legislative law and mandatory. And when I need an estate attorney, I have no intention of calling a medical professional… merely because Congress tells me to.
Your Media Matters headling proclaiming it is not mandatory is simply wrong via the HR3200 language, Larry. Sorry that they are unable to read and comprehend the obvious, and evidently they, too, think that legislative language is merely an “advisory brochure”. Per the language in HR3200, of which Palin was opposed:
Anything about “shall not be considered advanced care planning for purposes of applying the 5-year limitation” that doesn’t sound like it is mandatory? Or do you again think this is just friendly legislative advice?
How about this…
Apparently Media Matters has a problem interpreting proposed law. They don’t throw this stuff in there for fun, ya know.
I wanted to address this separately. Altho, in one way, it relates to me pointing out the obvious to you that legislation is not an “advisory brochure”, but law. If lawyers and professional consultants are acting otherwise (in service and in lawsuit before the bench in court), then that – again – is the fault of legislative language empowering them to do so.
I’m glad you agree that it’s part of the job. But the answer is not to redelegate that responsibility and allow for payment for unqualified individuals to do so via a mandate.
@mata:
Your distortion (which I’ll give you the benefit of the doubt is simply a result of you not understanding the bill) is breathtakingly inaccurate.
Your repeated assertions that there be mandatory end of life counseling was determined by the independent Politifact.com’s “Truth-o-meter” to be “PANTS ON FIRE UNTRUE”
http://www.politifact.com/truth-o-meter/statements/2009/jul/23/betsy-mccaughey/mccaughey-claims-end-life-counseling-will-be-requi/
You are not interpreting the language of the bill correctly. I’ll get to that below, but here’s what the AUTHOR (Oregon’s Rep Blumenauer) of Section 1233, HR3200 says about HIS OWN BILL:
http://blumenauer.house.gov/images/stories/documents/myth%20vs%20fact.pdf
Here’s the language of the Section. .
Larry’s comment: Let’s pause here. What does the above say? It doesn’t “mandate” anything whatsoever. There’s nothing in the language which mandates anyone to do anything. It simply means that, under “normal” circumstances, Medicare will pay a doctor (NOT A CLERK) for said doctor’s time in providing counseling in this area once every 5 years (this is a limitation, to prevent Medicare fraud, e.g. to prevent a doctor from having such a consultation with a given patient every week and billing Medicare every week. It says that the Medicare beneficiary is entitled to have Medicare pay for such a consultation every 5 years, if the patient wants it and the doctor wants to do it). This is NOT a mandate that such a consultation ever occur! Where in the world did you get that?
Now, the bill goes on to explain issues which are to be included in the counseling, IF the patient wishes to receive it and the doctor wishes to provide it. This sort of thing is absolutely usual and customary in description of Medicare benefits. When a doctor bills for a service, he uses a billing code. Each billing code provides language explaining what is to go into the service being billed. It means that, IF you wish to bill under this code, it is required that the services you provide include specific elements. Your services under the billing code are not limited to the specific elements, but must include them, if you wish to receive payment. They do not MANDATE that you provide these services, they simply say that, if you wish to be paid for the services you have to at least include the elements which are enumerated. In many cases, there are limitations as to how often you can provide the service and be billed for it. In the case in question, you can provide it only every 5 years, unless there has been some sort of important change in the patient’s medical condition to justify providing the service more often.
Continuing on with the language of the bill:
Let’s again pause here. You apparently feel that the above are strictly legal matters which either do not concern doctors or which doctors are not qualified to explain. I strongly disagree. In fact, I think that doctors are the professionals MOST qualified to explain these matters.
It comes up all the time: the patient is incapacitated. A decision needs to be made. The doctor can’t just make a command decision on the part of the patient (unless it’s a true life threatening emergency). Let’s say that the patient is mentally incapacitated (because of brain metastases, severe systemic infection, drugs, whatever). The doctor needs to do some sort of procedure (say, a spinal tap). Who is authorized to give permission to do this, on behalf of the patient. The point is, doctors are the best qualified professionals to explain to patients why they need durable powers of attorney and the powers and responsibilities of the person holding the durable power of attorney. The same thing with advance directives/living wills. Does the patient want feeding tubes, if required? What is a feeding tube? (nasogastric tube, gastrostomy tube, jejunostomy tube, etc. What lawyer is really qualified to explain these sorts of things?). Does the patient wish to be kept alive with total parenteral nutrition? What does that entail? What about a ventilator? Tracheostomy, in the event of airway compression by a cancer? All sorts of things — some general in nature and some specific to the patient’s own specific medical condition. It’s a way of allowing the patient to make as many choices as possible — in advance — as opposed to having to rely on the person designated by the patient to hold durable power of attorney.
Continuing:
Comment: These have nothing to do with death panels, euthanasia or any other such thing. It’s simply making sure that, if the doctor and patient want to do this counseling together and the doctor wants to bill for it, the doctor is required to provide the patient will all necessary and relevant information. Section D and E, in practice, would basically be providing the patient with a printed information sheet, listing resources, along with a verbal explanation. This section, along with the advance directives, living will, durable power of attorney, are specifically relevant in discussions between cancer patients and their oncologists, at a time when the oncologist feels that further available anti-cancer treatments (especially chemotherapy) are more likely to hurt the patient than help the patient.
The rest of the bill (section pertaining to end of life counseling is simply providing detailed guideline.
`
Now, Mata, you seem to have a problem with Nurse Practioners and Physician’s Assistants being eligible also for reimbursement. You may not be aware that both Nurse Practitioners and Physician’s Assistants are NOT some sort of low level clerical personal or aids: these are licensed professionals who are trained and licensed to provide many of the services traditionally provided by physicians. These professionals work semi-autonomously, albeit under the general supervision of a physician.
http://en.wikipedia.org/wiki/Nurse_practitioner
http://en.wikipedia.org/wiki/Physician_assistant
I’ll repeat again that Sarah Palin (and her supporters in this shameful hysterical scaremongering distortion) have done a profound disservice — potentially to hundreds of thousands of cancer patients covered under Medicare. The intention of the bill was honorable and noble: To compensate physicians for their time in provided needed counseling regarding end of life issues — again, these sorts of conversations most frequently involve cancer patients, in whom additional anti-cancer chemotherapy is more likely to harm the patient, rather than helping the patient.
– Larry Weisenthal/Huntington Beach, CA
@mata (#139, #140, #141): I wrote out a specific and detailed response, which, unfortunately, went to spam.
@Aqua (#137):
We were talking about comparative effectiveness research: why it is important and why, in it’s absence, doctors routinely play patients like violins, to the advantage of doctors and disadvantage of patients.
I’ve given the following example before, but I’d like to summarize it again, in the specific (new) context of comparative effectiveness research.
Example: Prostate Cancer
Background information is that prostate cancer is extremely common. Most men who make it to age 90 are incubating prostate cancer; few will die of it, however. Prostate cancer is a disease that many men live with, but relatively few die of. In the cases of those men who are destined to die of it, it has never been established definitively that there is any form of primary treatment (e.g. surgery, radiation) which will prevent death. It seems to be that prostate cancers which are destined to be aggressive may already have spread beyond the prostate (via the lymph nodes and/or blood stream) by the time it is first diagnosed.
Here’s how patients are played like violins and how they are played like violins.
You are a 60 year old man. You are having some problems with your love life, so you go to a urologist to have a medical evaluation (and maybe a prescription for Viagra). The urologist does as he is asked, but then suggests to you that you have a simple blood test for PSA (prostate specific antigen). If it’s elevated, then you could be harboring prostate cancer, which, he assures you, is “best caught early.”
Here’s the issue: Do you go along with him and have the test?
In the real world, almost certainly, you do. $ to the urologist (follow up visit for results). Anxiety and lost time to you. If the PSA is elevated, you then consent to have a needle biopsy of your prostate. $$$ to the urologist. Pain and suffering and expense for you. Then, let’s say, there is cancer in the biopsy needle. Of course, you want it to be treated. $$$$$$$ to the urologist. Pain, suffering, erectile dysfunction, urinary incontinence (could be permanent) to you. Perhaps $$ to the manufacture of Depends and $$$$, over time, to the manufacturer of Viagra. Additional $$$, for years’ worth of follow up visits. Perhaps additional surgeries to deal with complications.
Now, it turns out that the Europeans did a very nice comparative effectiveness study, published earlier this year. There was a similar study, performed and published at the same time, by a consortium of American investigators.
The American study showed no difference in death from prostate cancer in men who were screened with PSA testing and those who were not, despite the fact that the men who were screened had lots more biopsies, prostatectomies, complications from prostatectomies, radiation, complications of radiation, expense etc.
The European study showed a 20% decrease in deaths from prostate cancer in the group of men who were screened.
So, being a math whiz, when the urologist suggests getting a PSA test, you don’t just comply. It’s just a blood test, and you feel silly telling him that you won’t be able to make a decision until you research it. After all, you are already there. You may as well just have the stupid little blood test. But you still want some data. “What’s the evidence that this might help me?” you ask. Urologist doesn’t mention the negative American study. Such huge studies are never perfect. Since urologists don’t want their sacred cows killed and eaten, the pour over the negative study with a fine tooth comb, and they’ll always find a flaw upon which they can pounce (sort of like conservatives not liking the New England Journal of Medicine study showing that a large majority of the nation’s physicians would like to see health care reform and would like to see a public option in this reform — so they nit pick it to death).
With the American study duly nit picked, the urologist feels justified in not mentioning it to you. Instead, he quotes the European study:
“If we do this blood test, you’ve got a 20% less chance of dying of prostate cancer!”
He makes the sale. Simple blood test. 20% less chance of dying. Wow! What’s not to like.
Here’s what’s to like:
You have to do the blood test on 1450 men to prevent one death. In performing the test, you’ll get elevations which will prompt hundreds of biopsies which do NOT diagnose prostate cancer, but which do produce pain, suffering, inconvenience and $$$ for the urologist.
In 48 of these 1450 men, you will diagnose prostate cancer on the needle biopsy. With prostate cancer duly diagnosed, you will normally be directed into a radical prostatectomy (because it’s the urologist who is running the show). But, when you get the diagnosis, you might well tell the urologist that you want to think about it and research it and maybe get a second opinion. More $$ for other doctors. Maybe you opt for radiation therapy: external beam, radioactive “seed” implants, radioactive iridium wire implants, proton beam — lots of specialists to whom you may spread the $$ in getting the information to make your decision. Most men do end up with radical prostatectomies — radiation producing its own complications.
So you end up doing 48 radical prostatectomies (or 36 prostatectomies and 12 radiation therapies, or whatever) to prevent a single death from prostate cancer.
Now, would you really want to have the blood test, knowing that there was only a 1 in 1450 chance that it would help you and, if it were to help you, there would be a 47 in 48 chance that you’d get your prostate gland whacked out for nothing and only one chance in 48 that, if you had your prostate gland whacked out, it would help you?
If you give up red meat, there’s a greater than one chance in 48 that it will prolong your life. If you had to do one of the other, what would you give up: your prostate gland or red meat?
Freakonomics sort of stuff. They should put it in the next book.
But this is precisely why “comparative effectiveness research” is so important and should be supported by everyone.
Calling yourself a cello and not a violin. Priceless. Got a nice chuckle out of your humorous self-deprecation.
– Larry Weisenthal/Huntington Beach, CA
@Aqua (#137): This also went to spam.
A bit frustrating. I like to see them displayed right away, so that I can proof-read them for mistakes in spelling, grammar, and formatting. Easier to do these things in the final display mode than in the rough draft mode. – Larry W
General comment: I do a lot of ragging here, on my own profession (medicine in general and oncology in particular). I also do this in my various talks to physicians and oncologists. I recently received a video file of a talk I gave in Berlin, last March 19, 2009. I just posted this on Vimeo:
Vimeo allows for long format videos; Youtube limits to 10 minutes.
It’s 33 minutes long, but you can fast forward to exactly 6 minutes and 45 seconds in and get to a 3 minute section where I lob some very pointed criticisms at my profession, which are quite relevant to some matters discussed on this health care thread. The first couple minutes are a general introduction, then I go through some data, and then launch into the critique at 6 minutes and 45 seconds.
– Larry Weisenthal/Huntington Beach, CA
@openid.aol.com/runnswim: And you say my understanding of the bill language is “breathtaking”?
Let me put this simply, Larry. If you want the Medicare end of life consultations to be covered, you have to have them every five years (needed or not) or more often if there are health issues inbetween because of the built in “limitations”. Otherwise, that service is not covered.
That, my friend, is a mandate in order to obtain coverage. It is a “use it, or lose it” situation.
I said nothing about “forcing” people to sign living wills. What I said is that discussions about living wills and estate planning, wrapping up your final plans, is not the business of any medical professional. I stand by that. I also mentioned in a comment above that it was arrogant to assume the import of a medical provider in an individual’s life about these very personal issues.
It just so happens that on my last trip home, I helped my mother and father do this very same planning. It was extremely hard for her to do. And would have been that much more difficult trying to deal with these issues with a detached medical provider. Her primary doctor came into play merely when getting the appropriate paperwork to keep in an “emergency” file that I helped her set up… just so when the moment happened, and she was distraught, she could just grab a large file with several copies of living wills, documentation like birth certificates, my father’s service records, etal for EMTs, hospital personnel and/or funeral home representatives.
I have quite a few medical providers in my family. In one way, I admire their coolness in the face of severe illness and death. I do think that you have to become somewhat detached from the emotions of such in order to survive each day. It’s not like you are seeing people at their best moments in life.
However this detachment is the very reason I wholly disagree that medical providers are “the most qualified” to be end of life counselors. This is the job of family members, clergy, attorneys for most individuals. If they have no one, there are state services… or perhaps in rare instances may use their medical providers to perform that role.
But there is no getting around the actual bill language that there is a FIVE YEAR LIMITATION applied to the benefit. If you want to use that service, you MUST get the end of life consultation every five years.
Now, let’s talk about the “death panels”. I believed that Sarah was wrong in labeling these end of life counseling sessions as “death panels”. Especially since the actual death panels are going to be the increased rationing that occurs because of the government’s intent to hold the Medicare/Medicaid and planned public options in check. If they are going to reimburse below costs, there will be less state of the art equipment purchased and available. The “death panel” is going to be the IMAC… who will re’evaluate the Medicare costs every six months, and slash reimbursements and coverage in order to keep the system from becoming bankrupt.
However let’s go back to that “end of life counseling” MANDATE (if you want that service covered by Medicare). When this is implemented, can it be used to deny any treatment because an individual opted *not* to use the end of life coverage? That is the unknown. As you, yourself, noted, you wished that attorneys understood that explaining the risks/results of alternative treatments were actually part of a medical providers job. Obviously, with the way the legislation is so poorly written, there are loopholes that allow physicians to dodge that task as part of their service.
Thus may end up the same with this end of life counseling. Can they find a way to tie treatment to the fact that someone opts out of end of life counseling every five years (ore more)?
It comes down to this… you can’t guarantee it won’t anymore than I can’t guarantee you it will. But I’d say my concern about this has a better chance of happening than yours, based on past interpretations of legislative language in law.
Therefore I don’t consider that Palin did any damage to the end of life counseling issue, as you project so strongly. First of all, she was not alone in her opposition. Secondly, it just prevented doctors getting paid for something they should not be the lead counselor in anyway, IMHO. And having those services available thru family or even state programs that already exist saves wasted money on mandatory five year counseling (if they want the coverage for it). In other words, it’s just another needless “test”, so to speak, that drives up costs. Period.
Where in the world do you get that? It’s ridiculous. The 5 year thing just means that, if you are in a stable condition and are not having changes in your health, you are entitled to such a consultation every 5 years. It’s no different than Medicare saying you are entitled to have a colonoscopy every 5 years. There is no “mandate” to have a colonoscopy! And you can have a colonoscopy at any point in time that there is a change — let’s say new onset of blood in the stool. So then, you can have one, for examples, only 2 years after the previous one. But if it’s just a routine, screening test, you can’t get it more often than every 5 years. If you happen to miss a 5 year “anniversary,” you can still get one at 6 years or 7 years or 8 years. There’s no “use it or lose it.” What an absolutely ridiculous assertion! What would be the rationale? If the idea is to use this counseling to kill old people, then why punish them for being forgetful and missing a 5 year anniversary?
Firstly, there’s nothing in the bill about “estate planning!” That’s ridiculous. And do you have any idea what a living will is? It’s completely about what types of medical treatment are to be given and which are not. It’s all about medicine/health care. Do you want to have a “code” called if you have a cardiac arrest? What goes on in a “code?” Patients need to know this in order to decide. Do they ask their lawyer or do they ask their doctor? If they ask their lawyer, he’ll certainly bill them. How many lawyers really understand all the various medical procedures which might be provided in near end of life situations? Well enough to explain them to patients? Doctors understand the procedures which are in question and they are, by far, the best ones to explain these to patients. If they take the time to do this, they should be paid for their time, just as lawyers are certainly paid for their time. You were complaining on another thread about Medicare “squeezing” doctors. This is an attempt to compensate doctors, like oncologists, who have to do a whole lot of this stuff, which is important, and for which they are currently not being paid.
And if the patient doesn’t want a “medical provider” to advise them about medical procedures, THEY DON’T HAVE TO use this! But if they do want their medical provider to advise them about these MEDICAL issues, then the bill says that Medicare will pay the doctor — PROVIDED that this isn’t done more often than every 5 years (if no change in situation since the preceding counseling — again, this is simply to prevent Medicare fraud).
Larry Weisenthal/Huntington Beach CA
Let’s call this one the irony (or hypocrisy) of the day:
http://www.boston.com/news/politics/politicalintelligence/2009/11/gop_jettisons_a.html
They’ve had this since 1991! And they only noticed it now, less than a week after Pelosi successfully shepherded banning of abortion coverage into the Democratic health bill?
– LW/HB
Again, you did not read the language:
Again, I point out paragraph 1 as it relates to paragraph 3 above.
The way this language reads, if you want the consultations covered, there is a 5-year limitation… meaning use it, or lose it for coverage. I don’t care if colonoscopies are mandated or not. That’s nothing to do with *this* mandate. This, of course, is exactly the opposite of your personal interpretation:
I understand your interpretation of the language as it’s shared by every proponent of government provided health care, Larry. And in fact, the author of this bill section, Rep. Blumenauer, echoes that this was his intent with the language.
But again I remind you of your statement INRE doctors spending that extra 45 minutes to explain the risks/results of alternative treatment, and how lawyers exploit that in a court of law with vague legislative language.
Now one has to wonder, when implemented, who is correct? Would it have been exploited in the courts and denied coverage as interpreted as the same way I see it? Could they have potentially tied any treatment to the fact that someone refused such coverage and consultations?
The point is, the language is vague, and could be argued either way. And I’m generally one who tends to take the worst possible scenario as fact to avoid ugly surprises later.
It is also an unnecessary service/cost and provided by the wrong people, IMHO. It is not a service that is not unavailable via other avenues…. and for little to no cost.
Now let’s take another argument about this voluntary and/or mandated counseling that parallels with the unnecessary increased costs for services available for free elsewhere. This is from MedPage Today just a yesterday… pointing out that more pro-active patient mentality drives up costs unnecessarily.
Why, Larry, are you advocating increased costs for services offered for free elsewhere?
Now, let’s take another repercussion of such legislation… and this goes to the heart of your hatred for Sarah Palin. Quite frankly, I don’t think you understand her point. So let me reference some of her written testimony to the New York State Senate Aging Committee hearing.
Potential abuse, increased waste of funds for already provided services, and open to misinterpretation.
I rest my case.
And yes, I do know what a living will is… instructions INRE DNR. If that was Dad’s wishes, the last thing I wanted was for him to be taken to a hospital, put on life support, and force my mother to pull the plug. That is not something I’d want her to live with.
Powers of attorney (the 2nd arena of discussion) have everything to do with estate planning, unless that power of attorney is strictly limited to the living will. In fact, the legislative language specifically mentions durable power of attorney, which encompasses a considerably wider scope than merely DNR or medical decisions while incapacitated. It is not, as the legislation implies, merely a “health care proxy”. This advice can lead to empowering someone with far more decision making directives than the patient wants, and is best left to an attorney structuring just what they want that empowered person to be able to do.
Only an attorney can effectively limit the scope of power when constructing the POA, and therefore only an attorney should be providing legal advice. Doctors have no business practicing law.
A living will/DNR instruction isn’t the only “end of life” counseling, and includes minimally what to do about funeral arrangements, credit cards, social security notifications etal. The debris we leave behind in this world is immense.
Why should we drive up Medicare costs, paying medical professionals for small segment of genuine end of life counseling, when the larger scope of all involved is provided via other means? In fact, the legislation itself points out they have access to such via national toll-free hotlines, the advance care planning clearinghouses, and State legal service organizations.
Again why, Larry, are we adding to Medicare costs when this service is already available via free means?
This is all rather moot, when you think of it. This does not exist in the new bill, and these services are readily available via other channels. I see it as a waste of funding, and speaking with a medical professional about such is the last thing I’d want to do about such matters. All I’d want is, tell me what the treatments are (both what they would cover via Medicare, and what I could obtain OUTSIDE of Medicare, as the latter is often held back by the “wallet” mentality). Then let me make my decision.
I’ll figure out my own end of life plans without their help, thank you.
Mata, on this issue (the “mandate”) you are 100% wrong. Let me take you through it, step by step:
You quote me:
>>Larry W: The 5 year thing just means that, if you are in a stable condition and are not having changes in your health, you are entitled to such a consultation every 5 years. It’s no difference than Medicare saying you are entitled to have a colonoscopy every 5 years. There is no “mandate” to have a colonoscopy!<<
You say:
Yes I did.
What this means is that the rule for paying for end of life counseling does not apply to the initial physical examination and discussion for purposes of determining when the clock starts running on the proscription from providing counseling more than every 5 years. Let’s say that I get a new referral — breast cancer patient. During my initial evaluation, she asks me questions about living wills and advance treatment directives and so forth. I answer her questions. I take the total amount of time I spend with her (there is a formula for this) and bill medicare for a brief consultation or an extended consultation or a complex consultation or whatever. Even though we went over the living will/advance directive stuff, it doesn’t start the meter running. Let’s say that she decides not to have a living will.
Now, two years later, she hears something on Oprah which makes her decide that she might want to have a living will, after all. She makes an appointment with me solely to get more details on what sorts of specific medical procedures might come up in the future and which procedures she might want and which she might not want. So I spend 45 minutes explaining everything. Now, I am entitled to bill Medicare for end of life counseling, even though I did this 2 years previously, as part of my initial consultation, and even though it’s only 2 years later. However, at this point, the 5 year meter starts running. Let’s say that she goes ahead and gets with her lawyer and writes her living will. But then, another year or two later, she hears something on Larry King Live which makes her think she might want to revise her living will. She makes another appointment with me to discuss it. I can’t bill Medicare for end of life counseling, because it hasn’t been 5 years.
Now, let’s say that, one month after the above, she is passing dark urine and she comes in to see me and I diagnose metastatic breast cancer in her liver. She wants more counseling, because her condition has changed. I AM allowed to bill Medicare for this, even though it’s been less than 5 years since I last billed.
.
NO! You are WRONG! What that means is that the service is covered, PROVIDED THAT there has not been another such consultation within the 5 year period. Exactly like a colonoscopy. Your interpretation makes no sense at all. First, that’s not what the language says. Second, there would be no point in this. What would be the purpose? Saying that someone who got end of life counseling exactly 5 years ago was eligible for further coverage, while someone who got it 5 years and 1 day ago was not eligible. That’s stupid. The 5 year limit is simply to prevent overutilization and fraud. It makes sense for this and it’s precisely analogous to other Medicare benefits which are limited in the number of times you can get them within certain time periods (another good example is nursing home coverage).
Mata, you are totally WRONG on this. I say so. The Bill’s author says so. The language in the bill says so. Independent analysts say so. What you are saying makes no sense (“use it or lose it” for end of life counseling !!!??? That’s utterly and completely absurd, on it’s face and it’s not what the bill says).
Quoting me again:
>>But if they do want their medical provider to advise them about these MEDICAL issues, then the bill says that Medicare will pay the doctor — PROVIDED that this isn’t done more often than every 5 years<<
Well, duhh. That’s exactly what the language says!
No, it’s 100% clear. Especially in the context of established Medicare policy for similar issues (e.g. colonoscopy) and for the reason that your interpretation makes no sense whatsoever.
It’s all part of general end of life counseling which comes up, as I keep saying, most frequently in the context of a cancer patient failing all reasonable chemotherapy. The bill provides incentive for doctors to talk to their patients and explain that additional treatment is more likely to hurt them than to help them, as opposed to merely pushing in more poisons and avoiding the conversation. When you tell a patient that there are no more treatment options, he wants to know what this means and what is going to happen next and what are the issues and options. These take a long time to explain properly. They include both medical issues (for which it is entirely appropriate to compensate doctors) and legal issues (for which they may contact lawyers, who will certainly bill them for their time).
They aren’t the same services! The doctor doesn’t write the living will. He simply understands all the patient’s medical issues, understands what procedures and choices may be most likely to come up and which should be considered for the living will and advance directives. This is in the context of general medical counseling, as described above. So I think it’s great legislation, as it encourages Doctors to sit down and have difficult discussions with patients, as opposed to just pushing poisons and billing Medicare for said poisons.
But you can certainly argue everything on the basis of cost effectiveness. That’s not the issue. The issue here is Sarah Palin killing this legislation by claiming it’s about death panels. She’s an egotistical monster who is out of control and she’s harming thousands of cancer patients. So I’m a stakeholder in this.
But the proposed legislation wasn’t about “death panels!” There’s nothing at all in the language which is a threat to any Medicare patient. Yes, it’s true that Medicare can save money, when toxic and ineffective chemotherapy is not used. What happened is that very responsible legislators looked for ways to improve care, and provide cost savings at the same time. And they came up with a very responsible, compassionate piece of legislation, which also had the virtue of being potentially cost effective.
And a GOP hack decides to play politics, to the disadvantage of patients, by screaming “death panels,” and Palin picks up the megaphone and gets mega publicity for herself while directly harming thousands of future cancer patients. I consider her to be an egotistical monster of a politician. The worst kind of politician. The scaremongering type.
See my explanation, above. Absolutely everything in medicine can be misused. Tests can be misused. Surgery can be misused. Drugs can be misused. Counseling is part of medicine, and it can be misused as well. But it is doctors doing the counseling and doctors have no stake or incentive at all to kill patients prematurely. Doctors make money by providing services to patients, not by burying them.
Look at my post above on prostate cancer (#144). Let’s say that legislation was written to pay doctors to take the time to present all the data and explain the comparative effectiveness of screening versus no screening and surgery versus watchful waiting, so that patients could make informed choices. This would be a very good thing for the patient, in my opinion, and could also save Medicare some money. Sarah Palin could scream that this was an attempt to save money by denying patients potentially live saving cancer tests and treatment. It’s no different.
Oh, this is complete and utter crap. It’s a straw man. As I said, counseling could be misused, as can any other medical service. But there’s no incentive to the physician (who is doing the counseling) to die more quickly. And the language above pertaining to be “required to be counseled about the supposed benefits of killing oneself” are utterly outrageous! You should be ashamed of yourself for quoting that hysterical scaremongering. It’s hateful.
NO, IT IS NOT!! It’s exactly what it says it is: It provides reimbursement to doctors for taking the time to sit down with their patients to explain their medical situation and offer them the autonomy to make their own choices. A death panel makes decisions to kill people. There is absolutely nothing at all in the language of the bill which could begin to justify its characterization as setting up “death panels.”
And the bill was not withdrawn because of fears that it would be implemented incorrectly. It was withdrawn because of the political hysteria created by the shameless scaremogering of Sarah Palin.
1. Any medical procedure has the potential for abuse, leading to the premature death of patients. This proposed legislation has less potential for abuse and harm to the patient than most medical procedures for which Medicare pays. As I said before, there is no net financial incentive to a doctor to hasten the death of a patient. 2. These services are NOT “already provided!” Or, rather, they are greatly underprovided, because busy oncologists and other doctors, being human, don’t want to spend huge amounts of time doing things for which they won’t be paid, when the alternative is simply to go with the flow, provide more worthless and harmful treatment, and collect more money.
~~~
What went into my parent’s living wills were descriptions of which medical procedures they wished to receive and which they didn’t. Such descriptions can be either very simple, or very complex and detailed, depending on the specific clinical situation. It is usually preferable for the doctor to explain what procedures might come into consideration in a given patient’s situation.
.
You specifically said that doctors would be compensated for “estate planning.” No they won’t. They will be compensated for PROVIDING MEDICAL INFORMATION essential for construction of an appropriate durable power of attorney (i.e. what procedures should be part of advance directive — procedures that the doctor can foresee being required and on which the patient wants to decide in advance — and which procedures should be decided at a future time, with the person designated to have the durable power of attorney making the decisions, in the case the patient is incompetent. It doesn’t pay the doctor for writing the legal documents (the patient will still need a lawyer) but it does pay the doctor for providing medical information specific to the patient’s case which are required for informed planning.
The doctors aren’t being paid to practice law or draft legal documents. They are being paid to provide medical information necessary to make informed choices in drafting the legal documents.
No, and the doctor isn’t being paid to provide information about funeral arrangements and credit cards — only for providing medical information. This is 100% clear to everyone, except defenders of Sarah Palin.
The doctors are being paid for providing the overall medical aspects of end of life counseling — for providing counseling for specific medical issues relating to that specific patient, which no “toll free hotlines” are qualified to provide.
You totally don’t get it. Oncologists and other doctors who take care of terminally ill patients should be encouraged to counsel their patients, as opposed to simply performing revenue generating medical procedures on them. As part of the overall counseling, issues such as living wills and hospices come up. The bill was an honest effort to help patients and improve end of life care, which has the added benefit of saving money, when worthless treatments are not pursued. One can, again, have honest differences of opinion concerning the ultimate worth of the bill, to patients, doctors, and the system — but to scaremonger by characterizing the bill as an attempt to set up death panels and promote euthanasia is beyond outrageous, it is truly evil.
– Larry Weisenthal/Huntington Beach, CA
Larry, I swear this is my last post on a moot point of badly written, defunct legislation … which is why I was utterly opposed to it to begin with. You insist the law would work as intended, and I point out to you… and by your own admission.. that “intended” laws are abused by attorneys constantly.
If you portend you know how legislation will be implemented, and decided on in a court of law before it’s law, and before lawsuits arise, then so be it. How about a few stock tips for the rest of us, oh omnipotent one?
Yes, they should. And that should also be part of their current job, and not a separate payment for “end of life counseling”. If the patient is told of the types of treatments and their risks/results as part of that physician’s job, they already have enough information to make their informed decisions to take to an attorney to construct their living wills and wishes. You just support an extra charge to do this when frankly, you should be at the forefront arguing that doctors are not doing their full jobs when they do so automatically.
But then, you can’t…. can you? Because you, yourself, told us that the lawyers just don’t interpret that as part of a physician’s job. Must be some other explicitly clear legislation of intent that just doesn’t fly in the courts the way the authors intended, eh?
I do “totally get it”. I do encourage doctors to counsel patients on their options for treatment. Unlike you, I don’t think they should be paid extra for what they should do morally as part of their gig, and wrap up yet another revenue grabber by masking it as “end of life counseling” fee.
You may be correct that the bill was intended as “an honest effort” to make physicians responsible for their jobs. But I’ve never seen legislation make anyone especially due diligent if they aren’t inclined to do that already.
Then we get to Palin’s testimony where she plainly states that with government bureaucrats make medical decisions, it is a death panel… right on the heels of discussing the genuine “death panel”, Obama’s IMAC. I have constantly stated that I didn’t consider the end of life counseling the “death panel”, but I most certainly do the IMAC. Their entire existance is based on cutting reimbursements and coverage in order to keep the budget in line. As costs continue to rise… as will do since there is absolutely nothing built into this socialist utopian dream to reduce costs… trimming the fat and deciding who gets the coverage and who doesn’t is the job of the IMAC.
You read the testimony, insulted me for providing her quotes, then totally misconstrued what she was talking about. Congratulations. As I said, you really must learn to read slower.
Talk about hysterical scaremongering… congrats for that splendid demonstration of such. So Palin’s to blame for “harming thousands of cancer patients” because of no end of life counseling? That’s a hell of a leap, and a despicable transfer of responsibility. If anyone is harming “thousands of cancer patients”, it’s the “wallet oriented” doctors who do not consider it part of their job to counsel them on the risks/results unless they’re paid separately to do so.
I might also point out that Palin holds no power to vote on legislation, holds no elective office, and last I looked, it was Rush Limbaugh who was the head of the RNC per those with your mentality. The fact that you lay every bit of this at her feet reveals an extreme personal bias, an imagination usually found with paranoid mental disorders, and exhibit the quintessential liberal trait of “it’s always someone else’s fault”. Why did not your precious supermajority just keep it in, as they’ve kept the entire BS piece of legislation alive despite public opinion?
Get a grip, Larry. Honestly. You have an unhealthy fixation on a woman with very limited power. What Palin believes or doesn’t want is irrelevant when it’s exactly what Pelosi, Obama and Reid *do* want. Witness this is being pushed thru despite a more than health majority of Americans being opposed… just as we were opposed to the TARP bailout, the ARRA stimulus, the ominous Omnibus and the Cap and Tax. Yet you assume because Palin speaks, the Dems listen and cut it out of their bill? Seriously laughable.
Lastly, let’s not confuse Palin with myself. And I’m really fatigued with you constantly referring to me as a scaremonger… whether for things that I’ve said, or for things others have said. Frankly, Larry, each time you do that, you drop another notch in esteem with your Alinksy style debate tactics. It’s your distinct way of saying STFU. Playing that same game of personal assault, it’s people like you who will be content to be the death of America’s economics… and that’s not something I’m likely to ever forgive merely so you can “hope” for the social medical utopia you dream can happen – despite repeated history of it’s failure.
Reply to #150 went to spam.
I am sorry that I wasn’t able to proof check the formatting. I hope that it comes out OK, whenever it is retrieved and posted.
– larry w/HB
After 200 some-on posts by Larry, focused on NOTHING but this topic, I am now convinced he’s getting a kickback from the Whitehouse. NOBODY could be this damn adamant about such a losing POS as this bill without having something going on to make it worth it.
Or he’s sneaking meds.
Either way, it’s become pathetic.
Oh, by the way, scratch that 30,000 number of uninsured that Obama whittled down for a speech recently and don’t bother to pay any attention whatsoever to CBO cost estimates:
http://www.nytimes.com/2009/11/14/us/politics/14immig.html?_r=1&hp
That’s why they want this fiasco pushed through before the end of the year or by making this announcement now, they want to put a stake in it.
@mata (#153)
You gotta love the GOP. “Medicare is going broke!” Another “failed” government program.
Dems try to fix it: “Death panels!”
IMAC has nothing to do with death panels; it’s making reimbursement decisions on the basis of transparent, public deliberations (as opposed to private insurance and individual doctors, who make reimbursement and treatment decisions behind closed doors and inside closed skulls).
The “end of life counseling” had nothing to do with death panels; it was about reducing ineffective end of life treatments, improving quality of life at and of life, and also trying to control Medicare costs.
The legislation was good, clear legislation, as written. If there were any ambiguities, it would have been helpful to suggest changes in the language to clarify those ambiguities, instead of screaming “death panels.”
On one hand you maintain that doctors are leaving Medicare in droves, because they are being squeezed financially. On the other hand, you don’t think that a doctor should be paid for sitting down with a patient and telling him that his chemotherapy isn’t working anymore and further chemotherapy is much more likely to shorten his life than prolong his life and it is likely to make him feel worse and that, unfortunately, there are no more promising treatments left in the cupboard and said patient, of course, has lots of questions, and doctor patiently answers all of them and, in the course of this discussion, such things as advance directives and living wills and durable powers of attorney (“medical surrogate”) and hospice care come into it, and doctor explains the technicalities and limitations of foreseeable medical procedures, so that patient can make best informed decisions, and you feel that said doctor deserves no compensation for this, although you are only too happy to see said doctor get compensated for pushing chemotherapy and perhaps performing more futile surgery or giving more futile radiation.
The path of least resistance is just to keep treating, to the end. You get paid more; it takes less of your time; and it’s less stressful on you (no fun, at all, giving end of life counseling).
I have no problem at all with people pointing out ambiguous language, questioning cost effectiveness; taking the position that doctors shouldn’t be paid for thinking and talking but only paid for cutting and sewing and pushing drugs and directing radiation treatments (though the misincentive to provide treatment services as opposed to dispensing advice and counseling is at the heart of some of the most serious problems with the health care system).
You argue that the bill is imperfect and could be improved or isn’t necessary; that’s one thing.
Claiming that it’s about government bureaucrats deciding who’s going to live and who’s going to die and encouraging doctors to withhold effective treatment for the purpose of getting patients to die faster — that’s despicable.
And all Palin cared about was raising her profile, at the expense of tens of thousands of cancer patients. What she did was utterly despicable.
– Larry Weisenthal/Huntington Beach CA
Never once have I suggested that it was about doctors withholding treatment, encouraging patients to die faster. You put words into my mouth that I have never uttered. And that, Larry, is despicable. Again, you confuse me with someone else.
You totally misunderstand the IMAC legislation. Or perhaps you’ve never read it, as it’s a side bill with little fanfare. Have at it… Here’s the last proposed text I have. It is all about their power to recommend adjustments to reimbursements for everything from services to hospice care, prostetics, etal. When they cut percentage reimbursements, what exactly do you think happens to the insured patient… as well as the medical providers?
You say:
100% wrong, as you like to say. There is nothing public about the 5 man appointed panel, working behind closed doors with their recommendations first being reviewed by the Chief Actuary of the Centers for Medicare & Medicaid Services, and then passed on to the POTUS for approval. It can then only be reversed if the Senate can pull together a joint resolution within 30 days noting disapproval.
Yeah… real “transparent”, Larry.
As far as leaving Medicare in droves…. as I said, doctors should do this as part of their job. Period. I’m not going to argue that point any more, nor acquiesce that a way for them to pad their under cost reimbursements via an end of life counseling fee is the answer to service shortages. Fact is, real “reform” would be for better prices on equipment and supplies so their costs weren’t skyrocketing, or full reimbursement for their equipment and supplies. But add on extras to pad the loss is absurd.
If doctors choose “the path of least resistance” because it’s more money and less time consuming, *they*, not Palin, are the culprits. You blame her for their wallet mentality. That makes you despicable, and succumbing to the irresponsible shifting of blame, or the “it ain’t my fault” mentality. That is sheer, arrogant chutzpah.
@mata: Sigh, reply to #153 went to spam.
– Larry W/HB
@Patvann:
#1. I am a medic; so, of course, it’s the issue most important to me. Some on this blog only post on national defense or terrorism issues.
#2. You haven’t been around long enough. When I have the time and interest and when it’s topical, I like to debate economics, climate change, foreign policy, whatever.
But thanks for counting my posts. Nice to know that I’ve got such a loyal follower. 🙂
– Larry W/HB
Sorry Larry, I didn’t realized there was nothing else going on on this site, or even the planet important enough for you to avert your gaze. Hell it doesn’t even matter to you WHICH health payment-plan is at the fore, you support all of them, facts be damned!
Some “medics” might call it obsessive-compulsive.