“Monoclonal Antibody Treatments Save Lives,” announcedthe New York City Department of Health in an October 26 public notice. These treatments “are available and lifesaving,” the agency said, noting that they “have averted at least 1,100 hospitalizations and at least 500 deaths among people treated in New York City.” The agency urged the public to seek out these monoclonal antibody treatments as soon as possible: “When given early after symptom onset, mAb treatments can decrease the risk of hospitalization and death due to COVID-19, which is why it is crucial to get tested for COVID-19 as soon as symptoms begin – the sooner someone is tested, the sooner treatment can begin.”
The city’s health agency quoted its own Health Commissioner Dr. Dave A. Chokshi: “the science shows that monoclonal antibody treatments work and can make all the difference when it comes to the severity of COVID-19 illness.” It thus urged that “treatment should be given as soon as possible after someone tests positive for COVID-19.” Studies from Pfizer, cited by the agency, independently demonstrated just how effective the company’s antiviral treatment, called Paxlovid, can be: it “decreased Covid-19-linked hospitalisation or mortality risk from any cause by 88%.”
New York City Department of Health Press Release, Oct. 26, 2021
But with the Omicron variant now the dominant COVID strain in New York, both the city and state are facing severe shortages in the availability of effective antiviral monoclonal treatments. While Pfizer claimed its antiviral treatment would work against Omicron, the New York State Department of Health issued a memo to all health care providers this week warning that “Sotrovimab (Xevudy) is the only authorized monoclonal antibody product expected to be effective against the omicron variant.” Yet due to “a significant surge in cases and reduced effectiveness of existing therapeutics due to the omicron variant,” the agency warned that “supplies of oral antivirals will be extremely limited initially.” As of this week, the agency also said the same of its monoclonal antibody treatment: “supplies of Sotrovimab are extremely limited.”
These severe shortages mean that there will be far more people who are sick from COVID than there are available doses of antiviral and monoclonal antibodies treatment. That, in turn, requires that healthcare providers make decisions about who should be prioritized to receive such life-saving treatments and who should be deprioritized, and which factors ought to be used to determine priority.
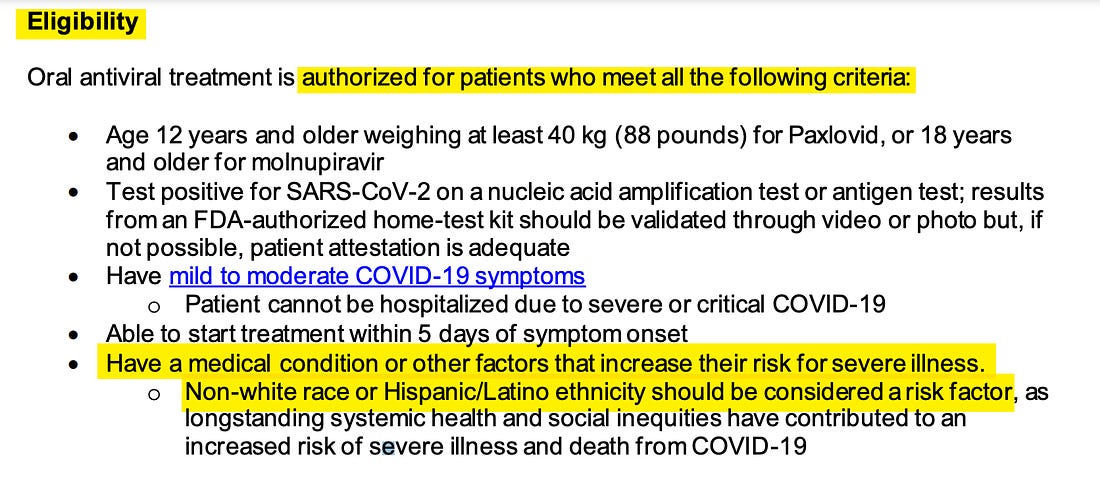
Before determining priority schemes, it must first be determined which groups of COVID patients are eligible at all to receive these potentially life-saving treatments and which from the start are declared ineligible. The state Department of Health memo sets out the list of all factors which must be met in order for a patient to be eligible. They include age (must be older than 12), COVID status (must have tested positive), and progression of the virus (must have “mild to moderate COVID-19 symptoms”).
Then there is an additional requirement that makes intuitive sense: the COVID patient must “have a medical condition or other factors that increase their risk for severe illness.” It makes sense that the government would seek to prioritize those who are at higher risk for developing severe illness.
But the policy then states that anyone who is non-white — regardless of age, health or underlying medical conditions — is automatically deemed to have met the requirement that one must have “a medical condition or other factors that increase their risk for severe illness” in order to receive this treatment (“Non-white race or Hispanic/Latino ethnicity should be considered a risk factor.”). That means that a healthy twenty-year-old Asian football player or a 17-year-old African-American marathon runner from a wealthy family will be automatically deemed at heightened risk to develop serious COVID illness — making them instantly eligible for monoclonal treatments upon testing positive and showing symptoms — while a White person of exactly the same age and health condition from an impoverished background would not be automatically eligible.
Eligibility requirements for treatments for the omicron strain of COVID, New York State Department of Health, Dec. 27, 2021
This policy was first flagged by New York journalist Karol Markowicz, whose Twitter summary described it as “white people need not apply.” That summary is not accurate. White people who are sick from COVID can still be eligible for antibody treatment, but only if they first demonstrate that they have “a medical condition that increase[s] their risk for severe illness.” But non-white people have the significant advantage of being automatically eligible without having to demonstrate that, since their non-white race is deemed to inherently constitute an increased risk of severe illness or death from COVID-19. In other words, when determining eligibility for life-saving treatments, New York state is explicitly prioritizing some races over others.
The rationale for using race to determine who is and is not eligible for life-saving COVID treatments is dubious in the extreme, to put it generously. The last passage of the New York Health Department’s memo states that “at this time, Sotrovimab (Xevudy) is the only authorized monoclonal antibody therapeutic that is expected to be effective against the omicron variant of SARS-CoV-2.” It directs that “Supplies of Sotrovimab are extremely limited and providers should adhere to NYS DOH prioritization guidance.”
That separate document establishes the official framework for determining not just eligibility but also prioritization in the event of limitations on the availability of COVID treatments. Entitled “Prioritization of Anti-SARS-CoV-2 Monoclonal Antibodies and Oral Antivirals for the Treatment of COVID-19 During Times of Resource Limitations,” the document details the triage procedures that should be used to determine which sick people get this treatment and which patients are denied it. “In times of limited supplies of monoclonal antibodies (mAbs) and oral antivirals (OAVs), providers should prioritize patients eligible for treatment based on their level of risk for progressing to severe COVID-19,” the memo states, adding: “in addition, the most efficacious products should be prioritized for patients with the highest risk for hospitalization and death.”
That document sets forth five different categories of patients who are entitled to priority when it comes to limited COVID treatment. The more risk factors a patient has, the higher priority they are assigned. As one would expect, COVID patients who are older, immunocompromised, and with “risk factors for severe illness” receive priority in the event of treatment shortages. But the priority scheme also directs that race be used as a critical metric: “non-white race or Hispanic/Latino ethnicity should be considered a risk factor, as longstanding systemic health and social inequities have contributed to an increased risk of severe illness and death from COVID-19.”
To justify this race-based priority scheme, the New York State memos rely on and cite two separate documents from the Centers for Disease Control (CDC). The first is entitled “People with Certain Medical Conditions,” and it lists the medical conditions that render a person “more likely to get severely ill from COVID-19.” On that list one finds the pathologies one would expect: cancer, diabetes, obesity, heart conditions and others. But the CDC also features race as a factor to consider when assessing risk:
Long-standing systemic health and social inequities have put various groups of people at increased risk of getting sick and dying from COVID-19, including many people from certain racial and ethnic minority groups and people with disabilities.
Studies have shown people from racial and ethnic minority groups are also dying from COVID-19 at younger ages. People in minority groups are often younger when they develop chronic medical conditions and may be more likely to have more than one condition
The document which the CDC cites is exclusively devoted to elaborating on its rationale for including race as a COVID risk factor. Entitled “Risk of Severe Illness or Death from COVID-19 — Racial and Ethnic Health Disparities,” it begins by asking: “Why are some racial and ethnic minority groups disproportionately affected by COVID-19?”
The factors which the CDC cites immediately make clear how warped it is to prioritize some racial groups over others when it comes to access to life-saving COVID treatments.
When you login first time using a Social Login button, we collect your account public profile information shared by Social Login provider, based on your privacy settings. We also get your email address to automatically create an account for you in our website. Once your account is created, you'll be logged-in to this account.
DisagreeAgree
Connect with
I allow to create an account
When you login first time using a Social Login button, we collect your account public profile information shared by Social Login provider, based on your privacy settings. We also get your email address to automatically create an account for you in our website. Once your account is created, you'll be logged-in to this account.
If you keep relying on “the authorities” to cure you of covid, you die.
Joe Biden’s Admin has even cornered the market on antiviral monoclonal treatments.
The shortage is manmade.
The rationing is also manmade.
There have been lots of other treatments for covid found to be effective either alone or in combination with one another.
ALL of them have been made difficult to get by the “vax or nothing,” Biden Admin.
Ronald Regan once said, “In this present crisis, government is not the solution to our problem; government is the problem.”
In the case of covid these words have proven to be true.
Take care of yourselves.
Don’t expect the gov’t to help you as if they care.
Spurwing Plover
2 years ago
New York was a Nice Place to live but its too bad Liberals ruined the place the same they do with all places that move into
I was wondering why vaccination status wasn’t mentioned by the NY fascists; the left, as they blame “Trump supporters” for the unvaccinated, fully recognizes that minorities, for various reasons, shun the vaccinations.
There is no “propagandizing against vaccination”. There are denouncements of illegal, fascist mandates. But, it was Democrats that denounced the vaccines.
So what you’re claiming now, Comrade Greggie, is that minorities who did not support or vote for Trump are following Trump supporters who are propagandizing against the vaccination?
Apparently there is no limits to the lies you are willing to tell. Which makes you pure scum.
And the FA village idiot because you truely believe you can convince people of logic to believe your lies.
That’s the narrative they give on CNN, but it’s not reality.
No one is against the vaccine. Sensible Americans are against sacrificing lives for some mass-psychosis obsession on a relatively weak and limited gene-therapy being treated as a 100% cure, will suppressing live-saving drugs because they don’t get corrupt companies like Merck rich.
You’re supporting the crony capitalist and the rich elite.
Trump threw the lobbyists out of the WH (something seldom covered on the fake-news sites you read), so they colluded to rig the election.



This article is all about how to survive covid once you are hospitalized. https://www.americanthinker.com/articles/2021/12/surviving_ten_days_with_covid_in_a_hospital.html
Hint: Sneak doses of ivermenctin inside your tissue box!
If you keep relying on “the authorities” to cure you of covid, you die.
Joe Biden’s Admin has even cornered the market on antiviral monoclonal treatments.
The shortage is manmade.
The rationing is also manmade.
There have been lots of other treatments for covid found to be effective either alone or in combination with one another.
ALL of them have been made difficult to get by the “vax or nothing,” Biden Admin.
Ronald Regan once said, “In this present crisis, government is not the solution to our problem; government is the problem.”
In the case of covid these words have proven to be true.
Take care of yourselves.
Don’t expect the gov’t to help you as if they care.
New York was a Nice Place to live but its too bad Liberals ruined the place the same they do with all places that move into
I was wondering why vaccination status wasn’t mentioned by the NY fascists; the left, as they blame “Trump supporters” for the unvaccinated, fully recognizes that minorities, for various reasons, shun the vaccinations.
They blame Trump supporters because it’s mainly Trump’s supporters who are propagandizing against vaccination.
There is no “propagandizing against vaccination”. There are denouncements of illegal, fascist mandates. But, it was Democrats that denounced the vaccines.
So what you’re claiming now, Comrade Greggie, is that minorities who did not support or vote for Trump are following Trump supporters who are propagandizing against the vaccination?
Apparently there is no limits to the lies you are willing to tell. Which makes you pure scum.
And the FA village idiot because you truely believe you can convince people of logic to believe your lies.
That’s the narrative they give on CNN, but it’s not reality.
No one is against the vaccine. Sensible Americans are against sacrificing lives for some mass-psychosis obsession on a relatively weak and limited gene-therapy being treated as a 100% cure, will suppressing live-saving drugs because they don’t get corrupt companies like Merck rich.
You’re supporting the crony capitalist and the rich elite.
Trump threw the lobbyists out of the WH (something seldom covered on the fake-news sites you read), so they colluded to rig the election.